
Immune Checkpoint Inhibitors and Their Cardiovascular Adverse Effects
 Ravi Kumar Paluri1,
Ravi Kumar Paluri1,  Yochitha Pulipati
Yochitha Pulipati Dileep Kumar Reddy Regalla
Dileep Kumar Reddy Regalla- 1Department of Hematology-Oncology, Atrium Health Wake Forest Baptist, Winston-Salem, NC, United States
- 2Department of Internal Medicine, Allegheny General Hospital, Pittsburgh, PA, United States
- 3Department of Hospital Medicine, OSF Saint Anthony Medical Center, Rockford, IL, United States
Immune checkpoint inhibitors (ICIs) have reshaped and have become a well-established treatment modality for multiple advanced-stage malignancies. ICIs block the immune system regulatory checkpoints, namely CTLA-4 and PD-1/PDL1, which provokes excess immune response against self-antigens. Immune modulation with ICIs can result in diverse immune-related adverse events targeting organ systems. Several cases of ICI-related cardiotoxicity were reported, while the actual incidence was likely underestimated due to heterogeneous clinical presentation. These include, but are not limited to, myocarditis, pericarditis, atherosclerosis, and arrhythmia. EKG, Troponin, Echocardiogram (TTE), and Cardiac MRI (CMRI) are indispensable diagnostic tools to aid in the management of cardiac adverse effects. Herein, we review the ICI-mediated cardiovascular adverse events, diagnosis, treatment strategies, and reintroduction of ICIs post-cardiotoxicity.
Introduction
Immune checkpoint inhibitors (ICIs) have changed the landscape of management of several cancers harnessing anti-tumor adaptive immunity by inhibiting key immune system inactivators such as CTLA-4, PD-1, and PDL-1. However, the robust immune response could act against self-antigens leading to significant toxicity. Cardiovascular toxicity is one of the primary forms of toxicity that often leads to treatment discontinuation. Most of the evidence on cardiovascular toxicity of ICIs has been limited to case series and systematic reviews, and little was known about ICI re-challenge post-cardiotoxicity. This review will highlight the available evidence on the most common ICI-related cardiotoxicity and their reintroduction.
Types of Cardiotoxicity
Ipilimumab (CTLA-4 inhibitor), Pembrolizumab/Nivolumab/Durvalumab (PD-1 inhibitors), and Atezolizumab (PD-L1 inhibitor) are the commonly used immune checkpoint inhibitors [1]. More recent ICIs include PD-1 inhibitors such as Dostarlimab [2] and Cemiplimab [3]. ICI-related cardiotoxicity has varied clinical manifestations, with myocarditis, pericarditis, cardiomyopathy, and arrhythmia being the commonly described ones. Other toxicities include vasculitis, hypertension, and atherosclerosis. A study has shown a three-fold higher risk of aortic plaque progression and coronary atherosclerosis leading to myocardial infarction and coronary revascularization [4]. Although myocarditis is potentially fatal, the treatment limitations of other cardiac manifestations have implications for further treatment continuation. According to a study, the most common cardiac complication was heart failure (17%), followed by myocarditis (15%) and pericarditis (13%) with myocarditis carrying the highest mortality rate [5]. Coronary artery vasculitis was reported in a few studies.
Myocarditis
CTLA-4 and PD-1, which are co-inhibitory molecules on T cells [6], are presumed to have a homeostatic role in the myocardium based on the pre-clinical data. For example, loss of CTLA-4 or PD-1 in mice induces spontaneous myocarditis [7, 8]. CTLA-4 is innately present on regulatory T cells, and inhibiting it promotes T cell stimulation [9]. Evolving data suggests that blocking PD-1 from binding with PD-L1 on cardiac myocytes triggers T cells against the myocardium [9]. Johnson et al hypothesized that a selective T-cell clone might attack the myocardium due to a common antigen between the tumor and myocardium, similar to the shared antigen theory [10]. Another theory is the development of autoantibodies causing myocarditis while on ICIs, as evidenced by pathology showing autoantibodies in a study [11, 12]. An autopsy study demonstrated predominant CD4+ T cell infiltration in the heart of patients treated with CTLA-4 inhibitor compared to CD8+ T cell infiltration in those treated with a PD-1 inhibitor [13]. It was proposed that pre-exposure to chemotherapy or radiotherapy could liberate cardiac antigens leading to enhanced ICI-related cardiotoxicity [14].
Incidence and prevalence of myocarditis varied greatly between studies owing to misclassification bias and lack of timely cardiac monitoring. The true incidence is difficult to estimate. For instance, a study has shown that concomitant treatment with Nivolumab and Ipilimumab causes myocarditis in 0.27% of patients vs. 0.06% in patients receiving only Ipilimumab [10]. In contrast, another study estimated the prevalence to be 1.14% [15]. A study estimated that there has been a 42% increase in the patient pool who qualify for ICIs from 2011 to 2018 [16]. It is unclear if this widened patient pool leads to an increased prevalence of myocarditis. The average onset time was 17 days between receiving ICIs and the development of myocarditis [10], in contrast to another study, which found that the average onset time was 34 days ranging from 1–3 months [15]. Another retrospective study demonstrated an average emergence time of 27 days, with 76% of cases reported within 6 weeks of starting treatment [17]. It is unclear if exposure to a different ICI, before the actual ICI that triggered the myocarditis, decreases the onset time of myocarditis, as evident in a few case reports [18].
Also, concomitant administration of CTLA-4 and PD-1/PDL-1 inhibition and diabetes mellitus were distinct predisposing factors for the development of ICI-associated myocarditis [15]. It is unclear if the type of cancer, pre-existing cardiac pathology, and autoimmune diseases increased the risk of myocarditis [19–22]. In a systematic review involving 88 cases, dyspnea (49%), followed by fatigue (25%), and chest pain (17%) were the most commonly reported symptoms [23–26]. Interestingly, smoldering myocarditis with little to no symptoms was reported [27].
Diagnosis of ICI-Related Myocarditis
In most cases of myocarditis, clinical picture and cardiac MRI (CMRI) help presume the diagnosis, though a gold standard procedure, endomyocardial biopsy (EMB) is seldom done due to its invasive nature [28].
Numerous definitions were proposed for the diagnosis of ICI-related myocarditis. Common terminology criteria for adverse events (CTCAE) has been historically used until Bonaca et al [29], put forward a criteria for standard assessments. More recently, the International Cardi-Oncology Society (IC-OS) proposed a criteria as in Table 1 below [30]. IC-OS criteria are binary, do not include PET scan, and rather include immune-related adverse events (irAEs) affecting other organ systems compared to criteria by Bonaca et al. In addition, a study has proposed including an onset time of symptoms of less than 3 months in the minor criteria to improve the specificity of IC-OS definition [31].
TABLE 1
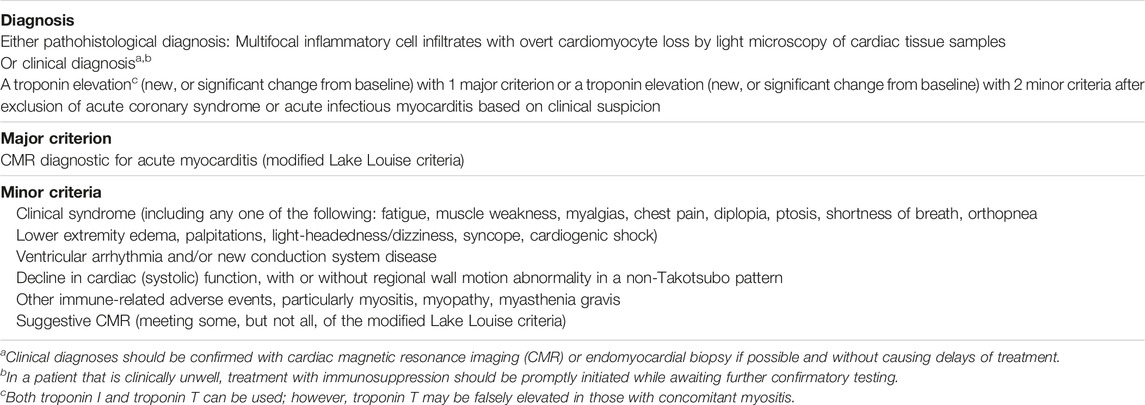
TABLE 1. [30] International Cardio-Oncology Society Consensus 2021 definition for immune checkpoint inhibitor myocarditis. Reprinted from defining cardiovascular toxicities of cancer therapies: An International Cardio-Oncology Society (IC-OS) consensus statement by Herrmann et al. (2021).
EKG: No specific finding on EKG was diagnostic of ICI myocarditis and majority of case reports showed widely variable findings like T wave inversions, sinus tachycardia, non-specific ST-T changes, QT prolongation, and even Torsades [32]. An abnormal ECG was found in 89% of myocarditis patients in a study [15]. Also, the worst prognostic features such as high grade heart block and ventricular arrhythmias were found in 28% and 22% of patients [26].
Cardiac Biomarkers
Troponin is crucial in the diagnosis of ICI-related myocarditis. Obtaining baseline troponin I is recommended in all patients before initiating ICIs [1]. A systematic review has shown elevated troponin in 42 out of 43 cases [26]. Normalization of troponin levels was observed in patients who responded to immunosuppressive therapy [27, 33, 34]. In contrast, an increasing troponin level is not always suggestive of or diagnostic of myocarditis, mandating comprehensive evaluation [35]. Nevertheless, ≥1.5 ng/mL troponin is linked to major adverse cardiac events [15]. As outlined in the IC-OS definition, troponin is a requisite for clinical diagnosis of ICI-related myocarditis. While studies suggested serial troponin monitoring for early diagnosis of ICI-related myocarditis, caution is advised in clinical interpretation due to significant false positives and inadvertent interruption in therapy [36]. In addition to troponin, CK-MB and CK levels were raised in many cases [18, 25, 26, 37]. Higher CK and CK-MB levels were linked to worse mortality [36]. Elevated BNP/NT pro-BNP [15, 25, 26, 43] and anti-striated muscle antibodies [19] are associated with the onset of myocarditis. Therefore, obtaining a baseline BNP/NT pro-BNP is recommended per European Society of Cardiology (ESC) guidelines [1].
Transthoracic Echocardiogram (TTE)
A multicentre registry showed preserved ejection fraction (EF) in 51% of cases [15], and it was unclear if preserved EF correlates well with a worse prognosis. A systematic review reported that 8 out of 13 cases with preserved EF died eventually [26]. It was also unclear if low EF leads to high mortality. In patients with a low risk of myocarditis, the global longitudinal strain could have a role, especially when EF is a poor diagnostic and prognostic indicator [38]. Also, a retrospective study of 101 patients showed that global longitudinal strain was lower in myocarditis compared to controls [39]. More recently, a study has shown that a reduction in longitudinal strain was linked to elevated troponin I levels [40]. A baseline TTE is recommended in patients who are at high risk of developing ICI-related myocarditis [1].
Cardiac MRI (CMRI)
CMRI is widely used to diagnose myocarditis. The characteristic findings include late gadolinium enhancement (LGE) with myocardial wall edema on T2-weighted imaging. A recent original research article involving six patients showed LGE in five out of six cases [18]. In contrast, another recent international registry study showed LGE in 48% of patients with ICI-associated myocarditis which warrants caution when relying on CMRI alone [41]. This low sensitivity could be explained by cases involving scattered to low-grade [40] myocardial inflammation [42].
Fluorodeoxyglucose-Positron Emission Tomography (FDG-PET)
Due to the lack of sensitivity of CMRI in cases with little to no myocardial inflammation, researchers have evaluated FDG-PET for its applicability. In a prospective study, FDG-PET complemented CMRI findings in 65 patients who were evaluated for possible myocarditis [43]. FDG-PET has been included in the diagnostic criteria by Bonaca et al.
Endomyocardial Biopsy
Endomyocardial biopsy has been considered the gold standard technique in diagnosing myocarditis from ICIs; however, this may not be feasible in all clinical scenarios. In a systematic review of 26 cases (14 cases underwent biopsy during angiography and 12 cases during autopsy), the biopsy showed predominantly lymphocytic myocarditis along with other cells. CD8+ve T cells were the major group of lymphocytes, along with occasional CD4+ve T cells [26]. Autopsy in a few case reports showed CD3+ T cells [44]. An autopsy showed lymphocytic myocarditis with patchy fibrosis with a confirmation of non-infectious etiology [45]. Despite being a gold standard diagnostic study, EMB could miss the diagnosis in patients presenting with focal myocardial inflammation.
Grades of Myocarditis
G1: Abnormal cardiac biomarker testing, including abnormal ECG.
G2: Abnormal screening tests with mild symptoms.
G3: Moderately abnormal testing or symptoms with mild activity.
G4: Moderate to severe decompensation, IV medication or intervention required, life-threatening conditions [46].
Management
The treatment of ICI-associated myocarditis is extrapolated from non-immunotherapy-related myocarditis. For example, ICI-associated myocarditis commonly presents in older populations, more likely to be associated with ventricular tachycardia/ventricular fibrillation/advanced heart block and higher mortality when compared to non-ICI myocarditis. Nevertheless, advanced age, co-morbidities, and advanced cancer could explain higher mortality [47].
Most case reports and systematic reviews initiated Methylprednisolone 1–2 mg/kg when myocarditis was suspected. In patients who worsen, few studies suggested the addition of Mycophenolate mofetil (MMF) or tacrolimus [48]. Also, in patients with limited response to initial doses of steroids, Methylprednisolone 1 gm/day can be considered [46]. Some experts and a few case reports have shown the benefit of using methylprednisolone 1 g daily upfront especially in patients in which high troponin corresponds to a higher risk of significant cardiac adverse effects [18, 19]. NCCN guidelines recommend a methylprednisolone pulse dose of 1 gm/day for G3 and G4 myocarditis, and steroid tapering over 4–6 weeks until the cardiac function returns to baseline [49]. ASCO guidelines recommend holding ICI for G1 and rechecking troponins 6 h after initial elevation. Resuming ICI could be considered after normalization of troponin. For Grade ≥2 myocarditis, ASCO recommends holding and initiating high-dose corticosteroids (1–2 mg/kg/day) within 24 h. In patients without an immediate response, pulse dose methylprednisolone 1g every day should be initiated [50]. Gradual tapering over 4–6 weeks is instituted when cardiac function returns to baseline. The flow chart (Figure 1) presented is derived from preceding data and expert consensus [50, 51].
FIGURE 1
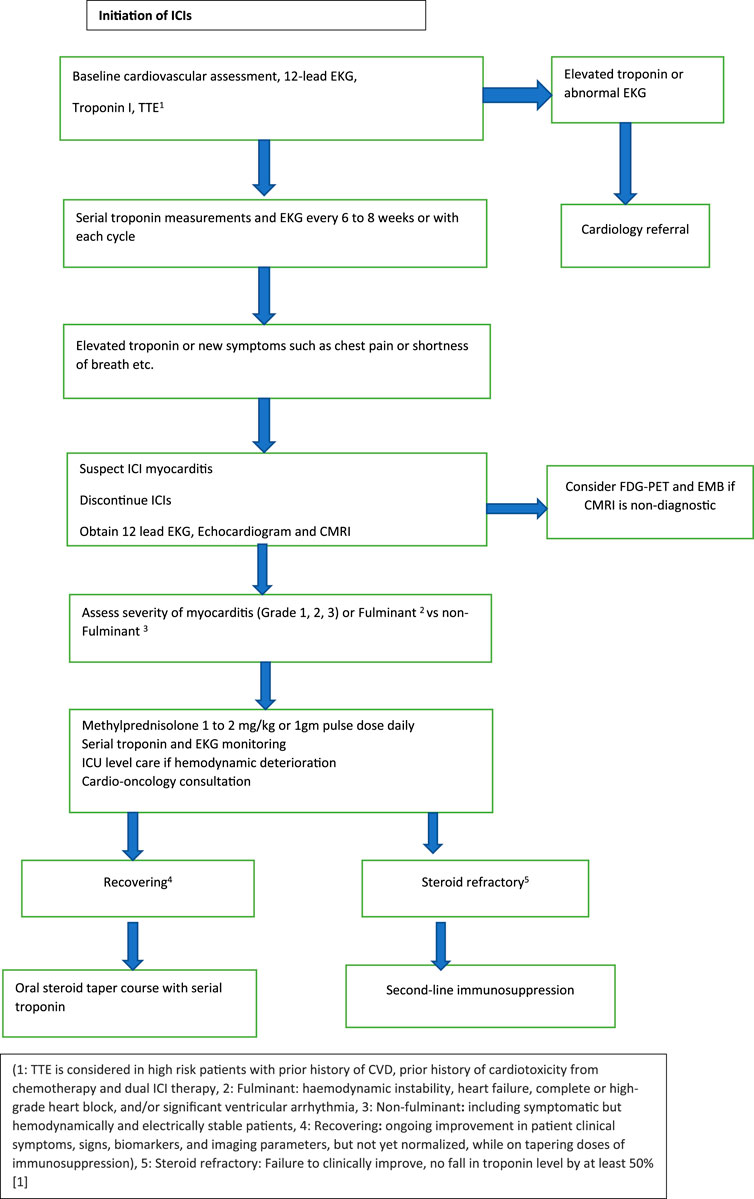
FIGURE 1. Management of ICI associated myocarditis.
Second-Line Immunosuppression
Various immunosuppressants have been studied for steroid-refractory cases. Steroid refractory myocarditis is defined as rising troponin or <50% reduction in troponin from peak with no clinical improvement [51]. NCCN recommends adding Antithymocyte globulin (ATG) or infliximab for G4 myocarditis if no improvement is seen within 24 h on steroids. However, it is important to note that infliximab is contraindicated in heart failure [49]. Limited evidence also suggests elevated cardiovascular death risk with infliximab [52]. In contrast, ESMO guidelines recommend adding tocilizumab or mycophenolate mofetil (MMF) as second-line agents followed by ATG or alemtuzumab or abatacept as third-line agents [51]. Additionally, ASCO guidelines recommend abatacept or alemtuzumab as additional options for life-threatening cases [50]. Resolution of steroid-refractory myocarditis from nivolumab with abatacept has been demonstrated in a case report [53]. Similarly, abatacept improved myocarditis from pembrolizumab in another case report, however, evidence is limited as the patient also received plasmapheresis [54]. Abatacept being a CTLA-4 agonist induces T cell anergy leading to suppression of inflammation, however, risks include infections and possible progression of cancer [53]. Alemtuzumab has been shown to have improved steroid refractory myocarditis from PD-1 inhibitor in a case report [55]. Alemtuzumab acts by killing peripheral immune cells however does not affect the bone marrow clone of immune cells [55]. Tocilizumab has also shown efficacy in the treatment of PD-1-associated myocarditis [56, 57]. Finally, plasmapheresis helps reduce inflammation by removing immune complexes and should be considered in life-threatening cases [58].
Outcome
In a systematic review of 99 cases, the overall case fatality rate was 35%. Mir et al reported that complete heart block and ventricular arrhythmias are associated with poor prognosis; interestingly, steroids showed no difference in survival. These patients were managed with immunosuppressive therapies, including MMF, ATG, and intravenous immunoglobulin (IVIG) to rescue 75% (9 out of 12 cases) [59]. Another systematic review reported that 31.1% of patients did not require hospitalization and the case fatality rate was 47.2%. Normalization of EKG correlated with clinical improvement [60, 61].
Role of Re-Challenging With ICI Following ICI-Associated Myocarditis
Hasson et al, described three cases of lung adenocarcinoma in which patients were treated with durvalumab, pembrolizumab, and atezolizumab, respectively [37]. In this case series, all three patients were diagnosed with myocarditis and treated with Prednisone. Two patients could sustain the ICI re-challenge upon resolution of myocarditis. However, unlike the other patients who had grade 1 and grade 2 severity, the third patient suffered a fatal outcome attributed to grade 3 severity. Guo et al described a case of stage 4 melanoma where Ipilimumab and Nivolumab were reintroduced after the resolution of atezolizumab-associated myocarditis, however, it was complicated by immune-mediated nephritis and stopped [10]. Few case reports demonstrated successful reintroduction of pembrolizumab and nivolumab [32, 62, 63]. Re-challenging was suggested in the above cases based on the response of malignancy to immunotherapy, normalization of ejection fraction, and cardiac biomarkers. Most importantly, the grade of myocarditis determines the recurrence of myocarditis, and co-treatment with low-dose maintenance prednisone may have favorable outcomes [25].
Per ASCO guidelines, it is recommended to discontinue ICI after a Grade ≥2 cardiovascular toxicity [91]. ESMO guidelines suggest permanent discontinuation of ICIs for steroid-resistant myocarditis or grade 4 myocarditis [51]. However, clinicians are posed with the challenge of making the decision of re-introducing the ICI, especially in the setting of a good tumor response. A careful multidisciplinary discussion and individualized approach in each case is warranted to make the choice. If the decision is made to re-challenge a patient, monotherapy with an alternative agent could be considered. For example, a study has demonstrated a successful rechallenge of pembrolizumab in patients who developed irAEs from combined CTLA-4 + PD-1 inhibitors. In this study, only 18% had recurrent irAEs among which none had myocarditis [64]. Similarly, a patient with pembrolizumab-induced grade 4 myocarditis was re-challenged with nivolumab at a lower dose with no recurrence [65]. In contrast, a pharmacovigilance analysis among 180 patients reported that re-challenging with the same ICI or same class ICI is associated with a lower risk of recurrent irAEs [66]. Systemic monitoring for cardiovascular symptoms, coupled with surveillance for asymptomatic disease with serial troponins and periodic cardiac imaging, is recommended [58]. Recurrence of myocarditis seems to be lower than colitis and hepatitis during re-challenge as demonstrated in a pharmacovigilance cohort study [67]. Table 2 outlines case scenarios where ICIs were reintroduced after myocarditis.
TABLE 2
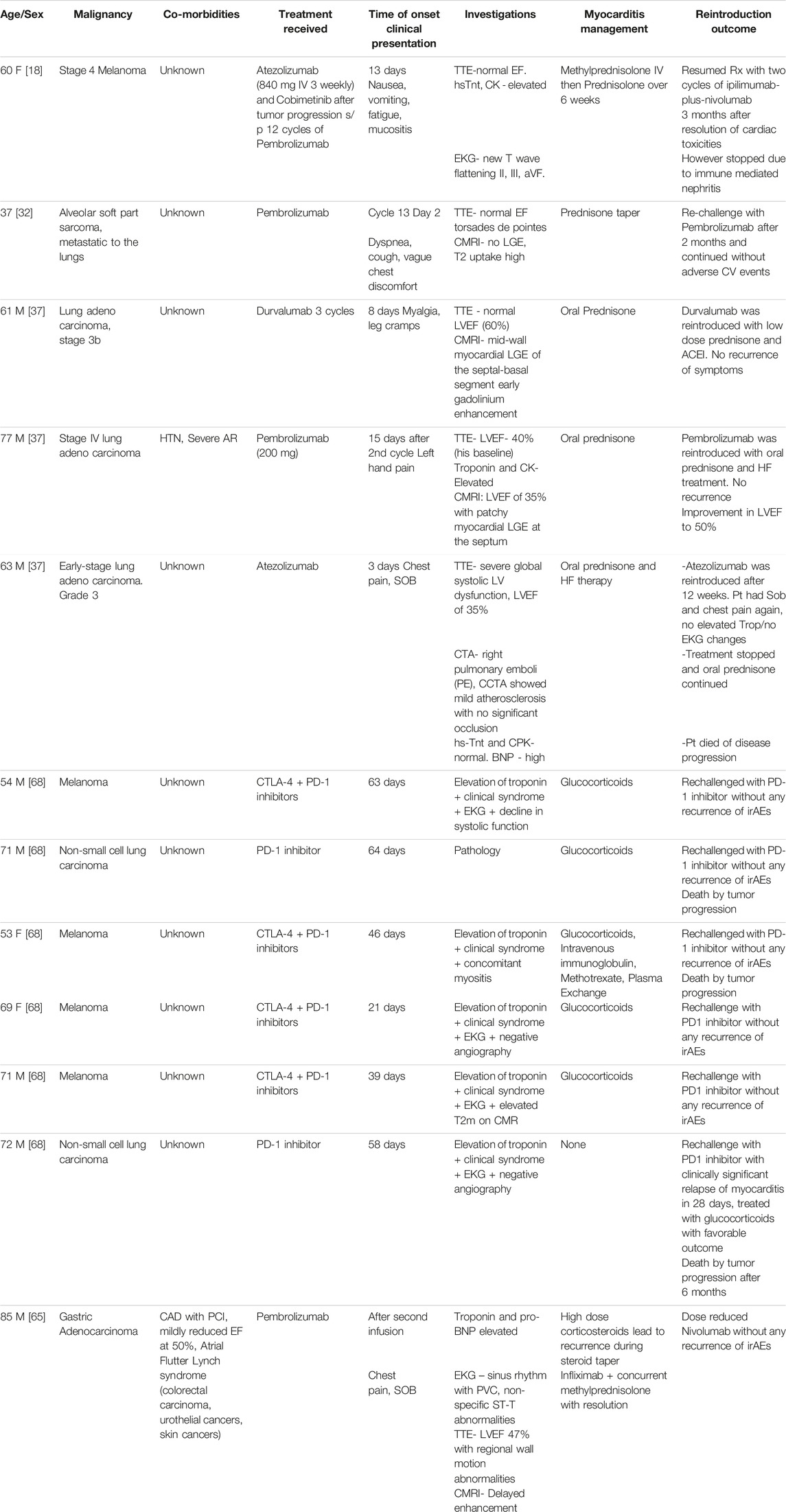
TABLE 2. ICI rechallenge for ICI-associated myocarditis.
Pericarditis
Pericardial disease from ICIs ranges from simple inflammation to fatal tamponade. Also, peri myocarditis/myopericarditis are other presentations associated with ICI [69].
ICI-associated pericarditis probably results from ICI-stimulated T cells against the pericardium leading to inflammation. The majority of these cases are associated with lung cancer patients [70]. The hypothesis behind this disproportionately high incidence of pericardial disease in lung cancer patients is the exposure of patients previously to radiotherapy. Theoretically, radiotherapy might expose the pericardial antigens leading to enhanced T-cell binding and inflammation [71]. Furthermore, CD 68+ve cells in pericardial fluid suggested macrophage impairment as a predisposing factor [72].
Hemodynamically significant pericardial effusions were reported in 0.38% (15/3,966) of patients treated with ICI [73]. The highest prevalence was noticed with Nivolumab (0.61%) thus far followed by pembrolizumab (0.19%) and atezolizumab (0.32%) [73]. An international database of patient case reports (WHO Vigibase) showed the average time to emergence of ICI-associated pericarditis as 30 days with a mortality of 20% [71]. A pharmacovigilance study showed that clinicians diagnosed 81% of pericarditis cases as high grade on presentation [70].
Clinical presentation of pericarditis could be cardiac symptoms like chest pain and SOB or non-specific ones such as myalgia and fatigue. EKG findings are usually non-specific, and TTE/MRI shows pericardial effusion and inflammation respectively. Also important is distinguishing pericarditis or pericardial effusion from pseudo-progression. Pseudo-progression is a condition with transient worsening of tumor status before resolution [74]. This pseudo-progression likely arises from the extensive inflammation generated from activated T cells against the tumor that leads to effusion [75, 76].
Histopathology
In most cases, pericardiocentesis revealed malignant cells along with inflammatory cells, commonly lymphocytes [77]. However, in a retrospective study on 15 patients with ICI-associated pericardial effusion, less than a third of patients had inflammatory cells in the pericardial fluid [73].
Grades of Pericarditis: (NCI-CTCAE v. 5.0)
G1: Asymptomatic with EKG or physical exam (example: pericardial rub) consistent with pericarditis.
G2: Symptomatic pericarditis (example: chest pain)
G3: Pericarditis with physiologic consequences.
G4: Pericarditis with life-threatening consequences needing urgent intervention G5: Death.
Management
A widely adopted treatment strategy that has proven effective in most instances was the temporary suspension of ICI along with the use of pericardiocentesis and corticosteroids. Additionally, successful results were reported with other treatments like MMF and TNF-alpha inhibitors. Corticosteroids alone were also associated with significant improvement [39]. Intrapericardial bleomycin (bleomycin: 15 mg/kg) [60], and pericardiectomy [55] were other commonly reported procedures. A systematic review of 28 cases of pericarditis showed that around 90% of Grade 3 to Grade 4 cases needed pericardiocentesis or pericardial window in addition to corticosteroids [78]. Based on the available evidence, ICIs could be continued for Grade 1 pericarditis. Corticosteroids are the cornerstone for Grade 2 to Grade 4 pericarditis and pericardiocentesis for moderate to large effusion. However, studying the role of non-steroidal anti-inflammatory drugs (NSAIDs) and Colchicine in ICI pericarditis is imperative. Table 3 outlines case scenarios where ICIs were reintroduced after pericarditis.
TABLE 3
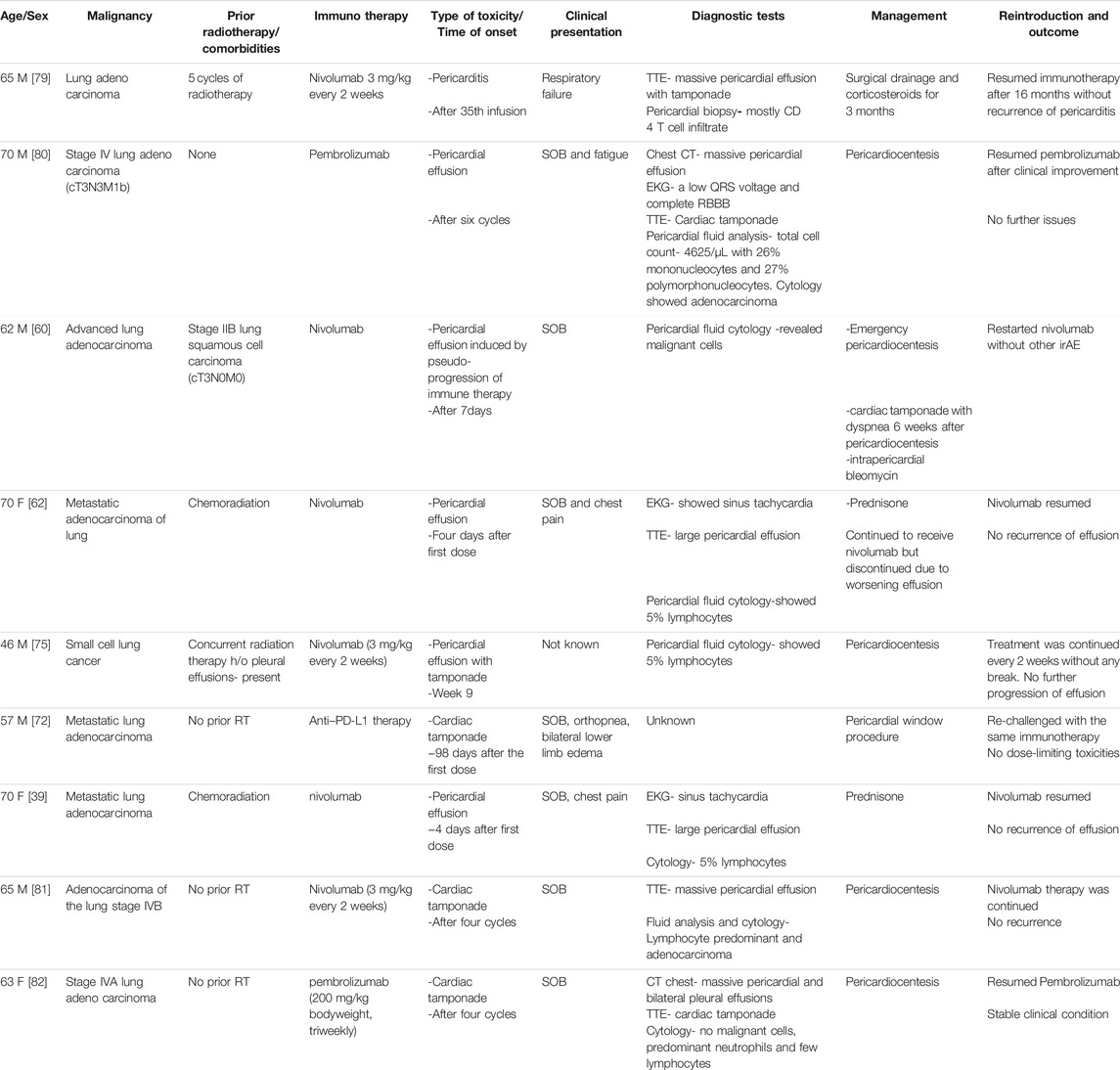
TABLE 3. ICI rechallenge for ICI associated pericarditis.
Atherosclerosis & Dyslipidemia
Multiple animal and human studies have demonstrated that PD-1, PD-L1, and CTLA-4 are down regulators of atherosclerosis [83, 84]. PD-1 deficiency could potentially increase cholesterol synthesis via gene regulation [85]. A meta-analysis has shown a significant association between ICIs and dyslipidemia leading to atherosclerosis and myocardial infarction (MI). Interestingly, dyslipidemia is this study’s most common adverse effect [86]. A single-center retrospective study has shown a three-fold higher risk of aortic plaque progression and coronary atherosclerosis leading to myocardial infarction, ischemic stroke, and coronary revascularization [4]. Another study demonstrated enhanced FDG-PET uptake in large arteries after ICI treatment signifying a pro-inflammatory state [87]. The above studies did not comment on previous radiotherapy administration, making the results questionable. Due to the probable association between ICIs and inflammation leading to atherosclerosis, treatment options to reduce this risk are of priority. Drobni et al revealed that the progression of aortic plaque while on ICIs was diminished with the usage of statin [4]. Statins enhance antigen presentation to CD4+ and CD8+ T cells by reducing protein prenylation in mice models [88]. This confers an enhanced inflammatory response and might lead to a synergistic action with ICIs. Notably, omori et al and cantini et al demonstrated increased response rate, PFS, and OS with statins while on anti-PD-1 therapy [89, 90]. A single-center retrospective observational study by Buti et al evaluated the effect of concomitant medications with ICI initiation on overall response rate (ORR), progression-free survival (PFS), and overall survival (OS). Statins were associated with better OS [91]. Another observational retrospective study by cortellini et al analyzed oncologic outcomes with ICIs while on concomitant medications, statins were associated with a better objective response rate [92]. A meta-analysis of cantini et al, buti et al, cortellini et al, and two other studies where statins and ICIs were used concomitantly, revealed better overall PFS and OS. Sub-group analysis, however, showed a correlation for better OS and PFS in cases where PD-1/PD-L1 inhibitors are used [93–95]. Similar to statins, PCSK-9 inhibitors also demonstrated synergistic action with PD-1 inhibitors by suppressing tumor growth in mouse models [96]. Further studies are necessary to validate the synergistic effect of statins and PCSK-9 inhibitors with ICIs. In addition, establishing the safety profile of statins while on ICIs is crucial due to the risk of adverse effects including but not limited to myopathy.
Arrhythmias
ICIs can lead to arrhythmias such as atrial fibrillation, supraventricular tachycardias, ventricular tachycardia, and heart blocks. It is important to note that these arrhythmias may arise independently due to various factors, such as concurrent myocarditis, pericarditis, or electrolyte abnormalities, and their relationship to ICIs is non-overlapping [70]. Ventricular arrhythmias are commonly seen in underlying myocarditis, making a correlation between ICIs and ventricular arrhythmias challenging [97].
Heart Failure & Cardiomyopathy
Cardiomyopathy resulting from ICIs can take two forms: inflammatory cardiomyopathy, typically associated with underlying myocarditis and non-inflammatory cardiomyopathy. Researchers hypothesize that the non-inflammatory heart failure syndrome is a delayed side effect [1]. Non-inflammatory cardiomyopathy presents as an exclusionary diagnosis where troponin is normal and there is no inflammation on CMRI [98]. Other presentations include Takotsubo cardiomyopathy [99]. The use of corticosteroids to treat non-inflammatory heart failure syndrome appears moot due to lack of inflammation, but further studies are necessary.
Vasculitis
Researchers hypothesize that the etiology of vasculitis stemming from ICIs comes from augmented inflammation within the blood vessels. For instance, in a study focused on Giant Cell Arteritis (GCA), it was observed that the expression levels of PD-1 and PD-L1 were diminished in the affected temporal arteries [100]. This indicates a potential link between ICIs and the onset of vasculitis. The deficiency of PD-1 and PD-L1 contributes to excess cytokine and T-cell aggregation response [101]. A pharmacovigilance study attributed 0.2% of irAEs to vasculitis, among other cardiotoxicities. Temporal arteritis was the most commonly reported event [70]. A case series reported that ICI-related vasculitis mainly involves large arteries, especially in the central nervous system [102]. Treatment mainly involves corticosteroids [103].
Arterial and Venous Thrombosis
Researchers hypothesize that a deficiency of PD-1, PD-L1, and CTLA-4 leads to enhanced inflammation culminating in arterial thrombosis (ATE) and venous thrombosis (VTE) [104]. A systematic review reported a VTE rate of 2.7% and an ATE rate of 1.1% [105]. In contrast, a recent meta-analysis did not report an increased risk of VTE in patients treated with ICIs [106]. Caution has to be exercised in attributing ICIs as the cause of thrombosis, as underlying cancer or paraneoplastic syndrome could be the primary driver of thrombosis. At this time, the role of prophylactic low-dose anticoagulation is unclear in patients treated with it. Further studies are warranted to develop a scoring system exclusively for ICI-treated patients to predict the necessity of prophylactic anticoagulation. ASCO guidelines stratify ICI-associated VTE into four grades [50].
G1: Superficial venous thrombosis.
G2: Uncomplicated deep vein thrombosis (DVT).
G3: Uncomplicated pulmonary embolism (PE).
G4: Life-threatening consequences from DVT or PE.
For G1, ASCO recommends continuing ICIs and close clinical surveillance. They recommend discontinuing ICIs and starting anticoagulation for G2 to G4 VTE. Re-initiation of ICIs might be an option after considering risks and benefits in the future for G2 to G4 toxicities [50].
Conclusion
Recognizing patients at risk, their ongoing monitoring and the chance to reintroduce immunotherapy presents significant challenges, particularly for those with a terminal prognosis. The evidence supporting the re-administration of ICIs for patients who experienced cardiac toxicity is scarce, and there is a lack of expert guidance in this area. Early and continuous interdisciplinary collaboration with cardiologists and oncologists is crucial to manage this situation effectively. Further research is required to understand the roles of cardiac MRIs and FDG-PETs, particularly given the limitations associated with invasive biopsy techniques. Besides myocarditis and pericarditis, it is important to identify and manage other potential ICI-related complications such as atherosclerosis, heart failure, and myocardial infarction. This attention to detail is vital in creating a comprehensive strategy for ICI-related cardiac events.
Author Contributions
This work was carried out in collaboration between all authors. RP gathered the literature data, wrote the initial manuscript draft. YP gathered the literature and refined the initial manuscript draft. DR put forward with the concept, reviewed and edited the final draft.
Conflict of Interest
RP is a consultant and adivisor for Exelixis, Ipsen and Seagen.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontierspartnerships.org/articles/10.3389/or.2023.11456/full#supplementary-material.
Supplementary Material S1 | (A) Main messages, (B) Multiple choice questions, (C) Key references, (D) Current research questions, (E) Answers.
References
1. Lyon, AR, López-Fernández, T, Couch, LS, Asteggiano, R, Aznar, MC, Bergler-Klein, J, et al. ESC Guidelines on Cardio-Oncology Developed in Collaboration With the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS): Developed by the Task Force on Cardio-Oncology of the European Society of Cardiology (ESC). Eur Heart J (2022) 43(41):4229–361. doi:10.1093/eurheartj/ehac244
2. Mirza, MR, Chase, DM, Slomovitz, BM, dePont Christensen, R, Novák, Z, Black, D, et al. Dostarlimab for Primary Advanced or Recurrent Endometrial Cancer. New Engl J Med (2023) 388(23):2145–58. doi:10.1056/nejmoa2216334
3. Gross, ND, Miller, DM, Khushalani, NI, Divi, V, Ruiz, ES, Lipson, EJ, et al. Neoadjuvant Cemiplimab for Stage II to IV Cutaneous Squamous-Cell Carcinoma. New Engl J Med (2022) 387(17):1557–68. doi:10.1056/nejmoa2209813
4. Drobni, ZD, Alvi, RM, Taron, J, Zafar, A, Murphy, SP, Rambarat, PK, et al. Association Between Immune Checkpoint Inhibitors With Cardiovascular Events and Atherosclerotic Plaque. Circulation (2020) 142(24):2299–311. doi:10.1161/circulationaha.120.049981
5. Master, SR, Robinson, A, Mills, GM, and Mansour, RP. Cardiovascular Complications of Immune Checkpoint Inhibitor Therapy. J Clin Oncol (2019) 37(15):2568. doi:10.1200/jco.2019.37.15_suppl.2568
6. Regalla, DKR, Williams, GR, and Paluri, Rk. Immune Checkpoint Inhibitors in the Management of Malignancies in Transplant Recipients. Postgrad Med J (2018) 94(1118):704–8. doi:10.1136/postgradmedj-2018-136081
7. Tivol, EA, Borriello, F, Schweitzer, A, Lynch, WP, Bluestone, JA, and Sharpe, AH. Loss of CTLA-4 Leads to Massive Lymphoproliferation and Fatal Multiorgan Tissue Destruction, Revealing a Critical Negative Regulatory Role of CTLA-4. Immunity (1995) 3(5):541–7. doi:10.1016/1074-7613(95)90125-6
8. Tarrio, ML, Grabie, N, Bu, D, Sharpe, AH, and Lichtman, AH. PD-1 Protects Against Inflammation and Myocyte Damage in T Cell-Mediated Myocarditis. J Immunol (2012) 188(10):4876–84. doi:10.4049/jimmunol.1200389
9. Tajiri, K, Aonuma, K, and Sekine, I Immune Checkpoint Inhibitor-Related Myocarditis. Jpn J Clin Oncol (2018) 48(1):7–12. doi:10.1093/jjco/hyx154
10. Johnson, DB, Balko, JM, Compton, ML, Chalkias, S, Gorham, J, Xu, Y, et al. Fulminant Myocarditis With Combination Immune Checkpoint Blockade. N Engl J Med (2016) 375(18):1749–55. doi:10.1056/nejmoa1609214
11. Xu, S, Sharma, UC, Tuttle, C, and Pokharel, S. Immune Checkpoint Inhibitors: Cardiotoxicity in Pre-Clinical Models and Clinical Studies. Front Cardiovasc Med (2021) 8:619650. doi:10.3389/fcvm.2021.619650
12. Tedeschi, A, Camilli, M, Ammirati, E, Gentile, P, Palazzini, M, Conti, N, et al. Immune Checkpoint Inhibitor-Associated Myocarditis: From Pathophysiology to Rechallenge of Therapy - A Narrative Review. Future Cardiol (2023) 19(2):91–103. doi:10.2217/fca-2022-0120
13. Reuben, A, Petaccia de Macedo, M, McQuade, J, Joon, A, Ren, Z, Calderone, T, et al. Comparative Immunologic Characterization of Autoimmune Giant Cell Myocarditis With Ipilimumab. Oncoimmunology (2017) 6(12):e1361097. doi:10.1080/2162402x.2017.1361097
14. Rubio-Infante, N, Ramírez-Flores, YA, Castillo, EC, Lozano, O, García-Rivas, G, and Torre-Amione, G. Cardiotoxicity Associated With Immune Checkpoint Inhibitor Therapy: A Meta-Analysis. Eur J Heart Fail (2021) 23(10):1739–47. doi:10.1002/ejhf.2289
15. Mahmood, SS, Fradley, MG, Cohen, JV, Nohria, A, Reynolds, KL, Heinzerling, LM, et al. Myocarditis in Patients Treated With Immune Checkpoint Inhibitors. J Am Coll Cardiol (2018) 71(16):A699–1764. doi:10.1016/s0735-1097(18)31240-3
16. Haslam, A, and Prasad, V Estimation of the Percentage of US Patients With Cancer Who Are Eligible for and Respond to Checkpoint Inhibitor Immunotherapy Drugs. JAMA Netw Open (2019) 2(5):e192535. doi:10.1001/jamanetworkopen.2019.2535
17. Moslehi, JJ, Salem, JE, Sosman, JA, Lebrun-Vignes, B, and Johnson, DB. Increased Reporting of Fatal Immune Checkpoint Inhibitor-Associated Myocarditis. The Lancet (2018) 391(10124):933. doi:10.1016/s0140-6736(18)30533-6
18. Guo, CW, Alexander, M, Dib, Y, Lau, PK, Weppler, AM, Au-Yeung, G, et al. A Closer Look at Immune-Mediated Myocarditis in the Era of Combined Checkpoint Blockade and Targeted Therapies. Eur J Cancer (2020) 124:15–24. doi:10.1016/j.ejca.2019.09.009
19. Ganatra, S, and Neilan, TG Immune Checkpoint Inhibitor-Associated Myocarditis. The Oncologist (2018) 23(8):879–86. doi:10.1634/theoncologist.2018-0130
20. Johnson, DB, Sullivan, RJ, and Menzies, AM Immune Checkpoint Inhibitors in Challenging Populations. Cancer (2017) 123(11):1904–11. doi:10.1002/cncr.30642
21. Johnson, DB, Sullivan, RJ, Ott, PA, Carlino, MS, Khushalani, NI, Ye, F, et al. Ipilimumab Therapy in Patients With Advanced Melanoma and Preexisting Autoimmune Disorders. JAMA Oncol (2016) 2:234. doi:10.1001/jamaoncol.2015.4368
22. Martinez-Calle, N, Rodriguez-Otero, P, Villar, S, Mejías, L, Melero, I, Prosper, F, et al. Anti-PD1 Associated Fulminant Myocarditis After a Single Pembrolizumab Dose: The Role of Occult Pre-Existing Autoimmunity. Haematologica (2018) 103(7):e318–e321. doi:10.3324/haematol.2017.185777
23. Semper, H, Muehlberg, F, Schulz-Menger, J, Allewelt, M, and Grohé, C. Drug-Induced Myocarditis After Nivolumab Treatment in a Patient With PDL1-Negative Squamous Cell Carcinoma of the Lung. Lung Cancer (2016) 99:117–9. doi:10.1016/j.lungcan.2016.06.025
24. Matson, DR, Accola, MA, Rehrauer, WM, and Corliss, RF. Fatal Myocarditis Following Treatment With the PD-1 Inhibitor Nivolumab. J Forensic Sci (2018) 63(3):954–7. doi:10.1111/1556-4029.13633
25. Tadokoro, T, Keshino, E, Makiyama, A, Sasaguri, T, Ohshima, K, Katano, H, et al. Acute Lymphocytic Myocarditis With Anti-PD-1 Antibody Nivolumab. Circ Heart Fail (2016) 9(10):e003514. doi:10.1161/circheartfailure.116.003514
26. Pradhan, R, Nautiyal, A, and Singh, S Diagnosis of Immune Checkpoint Inhibitor-Associated Myocarditis: A Systematic Review. Int J Cardiol (2019) 296:113–21. doi:10.1016/j.ijcard.2019.07.025
27. Norwood, TG, Westbrook, BC, Johnson, DB, Litovsky, SH, Terry, NL, McKee, SB, et al. Smoldering Myocarditis Following Immune Checkpoint Blockade. J ImmunoTherapy Cancer (2017) 5(1):91. doi:10.1186/s40425-017-0296-4
28. Kindermann, I, Barth, C, Mahfoud, F, Ukena, C, Lenski, M, Yilmaz, A, et al. Update on Myocarditis. J Am Coll Cardiol (2012) 59(9):779–92. doi:10.1016/j.jacc.2011.09.074
29. Bonaca, MP, Olenchock, BA, Salem, JE, Wiviott, SD, Ederhy, S, Cohen, A, et al. Myocarditis in the Setting of Cancer Therapeutics. Circulation (2019) 140(1):80–91. doi:10.1161/circulationaha.118.034497
30. Herrmann, J, Lenihan, D, Armenian, S, Barac, A, Blaes, A, Cardinale, D, et al. Defining Cardiovascular Toxicities of Cancer Therapies: An International Cardio-Oncology Society (IC-OS) Consensus Statement. Eur Heart J (2021) 43(4):280–99. doi:10.1093/eurheartj/ehab674
31. Deharo, F, Thuny, F, Cadour, F, Resseguier, N, Meilhac, A, Gaubert, M, et al. Diagnostic Value of the International Society of Cardio-Oncology Definition for Suspected Immune Checkpoint Inhibitor–Associated Myocarditis. J Am Heart Assoc (2023) 12(8):e029211. doi:10.1161/jaha.122.029211
32. Lee, DH, Armanious, M, Huang, J, Jeong, D, Druta, M, and Fradley, MG. Case of Pembrolizumab-Induced Myocarditis Presenting as Torsades de Pointes With Safe Re-Challenge. J Oncol Pharm Pract (2020) 26(6):1544–8. doi:10.1177/1078155220904152
33. Mehta, A, Gupta, A, Hannallah, F, Koshy, T, and Reimold, S. Myocarditis as an Immune-Related Adverse Event With Ipilimumab/Nivolumab Combination Therapy for Metastatic Melanoma. Melanoma Res (2016) 26(3):319–20. doi:10.1097/cmr.0000000000000251
34. Samara, Y, Yu, CL, and Dasanu, CA Acute Autoimmune Myocarditis and Hepatitis Due to Ipilimumab Monotherapy for Malignant Melanoma. J Oncol Pharm Pract (2019) 25(4):966–8. doi:10.1177/1078155218755868
35. Sarocchi, M, Grossi, F, Arboscello, E, Bellodi, A, Genova, C, Dal Bello, MG, et al. Serial Troponin for Early Detection of Nivolumab Cardiotoxicity in Advanced Non-Small Cell Lung Cancer Patients. The Oncologist (2018) 23(8):936–42. doi:10.1634/theoncologist.2017-0452
36. Puzanov, I, Subramanian, P, Yatsynovich, YV, Jacobs, DM, Chilbert, MR, Sharma, UC, et al. Clinical Characteristics, Time Course, Treatment and Outcomes of Patients With Immune Checkpoint Inhibitor-Associated Myocarditis. J ImmunoTherapy Cancer (2021) 9(6):e002553. doi:10.1136/jitc-2021-002553
37. Peleg Hasson, S, Salwen, B, Sivan, A, Shamai, S, Geva, R, Merimsky, O, et al. Re-Introducing Immunotherapy in Patients Surviving Immune Checkpoint Inhibitors-Mediated Myocarditis. Clin Res Cardiol (2020) 110:50–60. doi:10.1007/s00392-020-01648-3
38. Secchi, F, Monti, CB, Alì, M, Carbone, FS, Cannaò, PM, and Sardanelli, F. Diagnostic Value of Global Cardiac Strain in Patients With Myocarditis. J Comput Assist Tomogr (2020) 44(4):591–8. doi:10.1097/rct.0000000000001062
39. Awadalla, M, Mahmood, SS, Groarke, JD, Hassan, MZ, Nohria, A, Rokicki, A, et al. Global Longitudinal Strain and Cardiac Events in Patients With Immune Checkpoint Inhibitor-Related Myocarditis. J Am Coll Cardiol (2020) 75(5):467–78. doi:10.1016/j.jacc.2019.11.049
40. Tamura, Y, Tamura, Y, Takemura, R, Yamada, K, Taniguchi, H, Iwasawa, J, et al. Longitudinal Strain and Troponin I Elevation in Patients Undergoing Immune Checkpoint Inhibitor Therapy. JACC: CardioOncology (2022) 4(5):673–85. doi:10.1016/j.jaccao.2022.10.007
41. Zhang, L, Awadalla, M, Mahmood, SS, Nohria, A, Hassan, MZO, Thuny, F, et al. Cardiovascular Magnetic Resonance in Immune Checkpoint Inhibitor-Associated Myocarditis. Eur Heart J (2020) 41(18):1733–43. doi:10.1093/eurheartj/ehaa051
42. Friedrich, MG, Sechtem, U, Schulz-Menger, J, Holmvang, G, Alakija, P, Cooper, LT, et al. Cardiovascular Magnetic Resonance in Myocarditis: A JACC White Paper. J Am Coll Cardiol (2009) 53(17):1475–87. doi:10.1016/j.jacc.2009.02.007
43. Nensa, F, Kloth, J, Tezgah, E, Poeppel, TD, Heusch, P, Goebel, J, et al. Feasibility of FDG-PET in Myocarditis: Comparison to CMR Using Integrated PET/MRI. J Nucl Cardiol (2018) 25(3):785–94. doi:10.1007/s12350-016-0616-y
44. Hardy, T, Yin, M, Chavez, JA, Ivanov, I, Chen, W, Nadasdy, T, et al. Acute Fatal Myocarditis After a Single Dose of Anti-PD-1 Immunotherapy, Autopsy Findings: A Case Report. Cardiovasc Pathol (2020) 46:107202. doi:10.1016/j.carpath.2020.107202
45. Koelzer, VH, Rothschild, SI, Zihler, D, Wicki, A, Willi, B, Willi, N, et al. Systemic Inflammation in a Melanoma Patient Treated With Immune Checkpoint Inhibitors-An Autopsy Study. J ImmunoTherapy Cancer (2016) 4:13. doi:10.1186/s40425-016-0117-1
46. Brahmer, JR, Lacchetti, C, Schneider, BJ, Atkins, MB, Brassil, KJ, Caterino, JM, et al. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol (2018) 36(17):1714–68. doi:10.1200/jco.2017.77.6385
47. Veronese, G, and Ammirati, E Differences in Clinical Presentation and Outcome Between Immune Checkpoint Inhibitor-Associated Myocarditis and Classical Acute Myocarditis: Same Disease, Distinct Challenges to Face. Int J Cardiol (2019) 296:124–6. doi:10.1016/j.ijcard.2019.08.038
48. Haanen, J, Carbonnel, F, Robert, C, Kerr, K, Peters, S, Larkin, J, et al. Management of Toxicities From Immunotherapy: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann Oncol (2017) 28(4):iv119–iv142. doi:10.1093/annonc/mdx225
49. Thompson, JA, Schneider, BJ, Brahmer, J, Andrews, S, Armand, P, Bhatia, S, et al. Management of Immunotherapy-Related Toxicities, Version 1.2019, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Cancer Netw (2019) 17(3):255–89. doi:10.6004/jnccn.2019.0013
50. Schneider, BJ, Naidoo, J, Santomasso, BD, Lacchetti, C, Adkins, S, Anadkat, M, et al. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: ASCO Guideline Update. J Clin Oncol (2021) 39(36):4073–126. doi:10.1200/jco.21.01440
51. Haanen, J, Obeid, M, Spain, L, Carbonnel, F, Wang, Y, Robert, C, et al. Management of Toxicities From Immunotherapy: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up. Ann Oncol (2022) 33(12):1217–38. doi:10.1016/j.annonc.2022.10.001
52. Cautela, J, Zeriouh, S, Gaubert, M, Bonello, L, Laine, M, Peyrol, M, et al. Intensified Immunosuppressive Therapy in Patients With Immune Checkpoint Inhibitor-Induced Myocarditis. J ImmunoTherapy Cancer (2020) 8(2):e001887. doi:10.1136/jitc-2020-001887
53. Salem, J-E, Allenbach, Y, Vozy, A, Brechot, N, Johnson, DB, Moslehi, JJ, et al. Abatacept for Severe Immune Checkpoint Inhibitor–Associated Myocarditis. New Engl J Med (2019) 380(24):2377–9. doi:10.1056/nejmc1901677
54. Liu, S, Chan, J, Brinc, D, Gandhi, S, Izenberg, A, Delgado, D, et al. Immune Checkpoint Inhibitor-Associated Myocarditis With Persistent Troponin Elevation Despite Abatacept and Prolonged Immunosuppression. JACC: CardioOncology (2020) 2(5):800–4. doi:10.1016/j.jaccao.2020.10.013
55. Esfahani, K, Buhlaiga, N, Thébault, P, Lapointe, R, Johnson, NA, and Miller, WH. Alemtuzumab for Immune-Related Myocarditis Due to PD-1 Therapy. N Engl J Med (2019) 380(24):2375–6. doi:10.1056/nejmc1903064
56. Wang, H, Tian, R, Gao, P, Wang, Q, and Zhang, L. Tocilizumab for Fulminant Programmed Death 1 Inhibitor–Associated Myocarditis. J Thorac Oncol (2020) 15(3):e31–e32. doi:10.1016/j.jtho.2019.09.080
57. Doms, J, Prior, J, Peters, S, and Obeid, M. Tocilizumab for Refractory Severe Immune Checkpoint Inhibitor-Associated Myocarditis. Ann Oncol (2020) 31(9):1273–5. doi:10.1016/j.annonc.2020.05.005
58. Patel, RP, Parikh, R, Gunturu, KS, Tariq, RZ, Dani, SS, Ganatra, S, et al. Cardiotoxicity of Immune Checkpoint Inhibitors. Curr Oncol Rep (2021) 23(7):79. doi:10.1007/s11912-021-01070-6
59. Mir, H, Alhussein, M, Alrashidi, S, Alzayer, H, Alshatti, A, Valettas, N, et al. Cardiac Complications Associated With Checkpoint Inhibition: A Systematic Review of the Literature in an Important Emerging Area. Can J Cardiol (2018) 34(8):1059–68. doi:10.1016/j.cjca.2018.03.012
60. Reddy, N, Moudgil, R, Lopez-Mattei, JC, Karimzad, K, Mouhayar, EN, Somaiah, N, et al. Progressive and Reversible Conduction Disease With Checkpoint Inhibitors. Can J Cardiol (2017) 33(10):1335.e13–1335.e15. doi:10.1016/j.cjca.2017.05.026
61. Gibson, R, Delaune, J, Szady, A, and Markham, M. Suspected Autoimmune Myocarditis and Cardiac Conduction Abnormalities With Nivolumab Therapy for Non-Small Cell Lung Cancer. BMJ Case Rep (2016) 2016:bcr2016216228. doi:10.1136/bcr-2016-216228
62. Shaheen, S, Mirshahidi, H, Nagaraj, G, and Hsueh, CT. Conservative Management of Nivolumab-Induced Pericardial Effusion: A Case Report and Review of Literature. Exp Hematol Oncol (2018) 7:11. doi:10.1186/s40164-018-0104-y
63. Heinzerling, L, Ott, PA, Hodi, FS, Husain, AN, Tajmir-Riahi, A, Tawbi, H, et al. Cardiotoxicity Associated With CTLA4 and PD1 Blocking Immunotherapy. J ImmunoTherapy Cancer (2016) 4:50. doi:10.1186/s40425-016-0152-y
64. Pollack, MH, Betof, A, Dearden, H, Rapazzo, K, Valentine, I, Brohl, A, et al. Safety of Resuming Anti-PD-1 in Patients With Immune-Related Adverse Events (irAEs) During Combined Anti-CTLA-4 and Anti-PD1 in Metastatic Melanoma. Ann Oncol (2018) 29(1):250–5. doi:10.1093/annonc/mdx642
65. Eslinger, C, Walden, D, Barry, T, Shah, S, Samadder, NJ, and Bekaii-Saab, TS. Rechallenge With Switching Immune Checkpoint Inhibitors Following Autoimmune Myocarditis in a Patient With Lynch Syndrome. J Natl Compr Cancer Netw (2023) 21(9):894–9. doi:10.6004/jnccn.2023.7029
66. Allouchery, M, Lombard, T, Martin, M, Rouby, F, Sassier, M, Bertin, C, et al. Safety of Immune Checkpoint Inhibitor Rechallenge After Discontinuation for Grade ≥2 Immune-Related Adverse Events in Patients With Cancer. J Immunother Cancer (2020) 8(2):e001622. doi:10.1136/jitc-2020-001622
67. Dolladille, C, Ederhy, S, Sassier, M, Cautela, J, Thuny, F, Cohen, AA, et al. Immune Checkpoint Inhibitor Rechallenge After Immune-Related Adverse Events in Patients With Cancer. JAMA Oncol (2020) 6(6):865–71. doi:10.1001/jamaoncol.2020.0726
68. Coustal, C, Vanoverschelde, J, Quantin, X, Lesage, C, Michot, JM, Lappara, A, et al. Prognosis of Immune Checkpoint Inhibitors-Induced Myocarditis: A Case Series. J Immunother Cancer (2023) 11(5):e004792. doi:10.1136/jitc-2022-004792
69. Chen, DY, Huang, WK, Chien-Chia Wu, V, Chang, WC, Chen, JS, Chuang, CK, et al. Cardiovascular Toxicity of Immune Checkpoint Inhibitors in Cancer Patients: A Review When Cardiology Meets Immuno-Oncology. J Formos Med Assoc (2020) 119:1461–75. doi:10.1016/j.jfma.2019.07.025
70. Salem, JE, Manouchehri, A, Moey, M, Lebrun-Vignes, B, Bastarache, L, Pariente, A, et al. Cardiovascular Toxicities Associated With Immune Checkpoint Inhibitors: An Observational, Retrospective, Pharmacovigilance Study. Lancet Oncol (2018) 19(12):1579–89. doi:10.1016/s1470-2045(18)30608-9
71. Escudier, M, Cautela, J, Malissen, N, Ancedy, Y, Orabona, M, Pinto, J, et al. Clinical Features, Management, and Outcomes of Immune Checkpoint Inhibitor-Related Cardiotoxicity. Circulation (2017) 136(21):2085–7. doi:10.1161/circulationaha.117.030571
72. Altan, M, Toki, MI, Gettinger, SN, Carvajal-Hausdorf, DE, Zugazagoitia, J, Sinard, JH, et al. Immune Checkpoint Inhibitor-Associated Pericarditis. J Thorac Oncol (2019) 14(6):1102–8. doi:10.1016/j.jtho.2019.02.026
73. Palaskas, N, Morgan, J, Daigle, T, Banchs, J, Durand, JB, Hong, D, et al. Targeted Cancer Therapies With Pericardial Effusions Requiring Pericardiocentesis Focusing on Immune Checkpoint Inhibitors. Am J Cardiol (2019) 123(8):1351–7. doi:10.1016/j.amjcard.2019.01.013
74. Zhou, YW, Zhu, YJ, Wang, MN, Xie, Y, Chen, CY, Zhang, T, et al. Immune Checkpoint Inhibitor-Associated Cardiotoxicity: Current Understanding on its Mechanism, Diagnosis and Management. Front Pharmacol (2019) 10:1350. doi:10.3389/fphar.2019.01350
75. Kolla, BC, and Patel, MR Recurrent Pleural Effusions and Cardiac Tamponade as Possible Manifestations of Pseudoprogression Associated With Nivolumab Therapy-A Report of Two Cases. J ImmunoTherapy Cancer (2016) 4:80. doi:10.1186/s40425-016-0185-2
76. Tocchetti, CG, Galdiero, MR, and Varricchi, G Cardiac Toxicity in Patients Treated With Immune Checkpoint Inhibitors: It Is Now Time for Cardio-Immuno-Oncology. J Am Coll Cardiol (2018) 71(16):1765–7. doi:10.1016/j.jacc.2018.02.038
77. Khunger, A, Battel, L, Wadhawan, A, More, A, Kapoor, A, and Agrawal, N. New Insights Into Mechanisms of Immune Checkpoint Inhibitor-Induced Cardiovascular Toxicity. Curr Oncol Rep (2020) 22(7):65. doi:10.1007/s11912-020-00925-8
78. Inno, A, Maurea, N, Metro, G, Carbone, A, Russo, A, and Gori, S. Immune Checkpoint Inhibitors-Associated Pericardial Disease: A Systematic Review of Case Reports. Cancer Immunol Immunother (2021) 70(10):3041–53. doi:10.1007/s00262-021-02938-z
79. Saade, A, Mansuet-Lupo, A, Arrondeau, J, Thibault, C, Mirabel, M, Goldwasser, F, et al. Pericardial Effusion Under Nivolumab: Case-Reports and Review of the Literature. J ImmunoTherapy Cancer (2019) 7(1):266. doi:10.1186/s40425-019-0760-4
80. Tachihara, M, Yamamoto, M, Yumura, M, Yoshizaki, A, Kobayashi, K, and Nishimura, Y. Non-Parallel Anti-Tumour Effects of Pembrolizumab: A Case of Cardial Tamponade. Respirology Case Rep (2019) 7(3):e00404. doi:10.1002/rcr2.404
81. Yamasaki, M, Daido, W, Saito, N, Funaishi, K, Okada, T, Kawamoto, K, et al. Pericardial Effusion With Tamponade in Lung Cancer Patients During Treatment With Nivolumab: A Report of Two Cases. Front Oncol (2019) 9:4. doi:10.3389/fonc.2019.00004
82. Harada, K, Ogasawara, M, Shido, A, Meno, A, Oda, S, Yoshida, S, et al. Pericardial Tamponade During Pembrolizumab Treatment in a Patient With Advanced Lung Adenocarcinoma: A Case Report and Review of the Literature. Thorac Cancer (2020) 11(5):1350–3. doi:10.1111/1759-7714.13399
83. Fernandez, DM, Rahman, AH, Fernandez, NF, Chudnovskiy, A, Amir, ED, Amadori, L, et al. Single-Cell Immune Landscape of Human Atherosclerotic Plaques. Nat Med (2019) 25(10):1576–88. doi:10.1038/s41591-019-0590-4
84. Gotsman, I, Grabie, N, Dacosta, R, Sukhova, G, Sharpe, A, and Lichtman, AH. Proatherogenic Immune Responses Are Regulated by the PD-1/PD-L Pathway in Mice. J Clin Invest (2007) 117(10):2974–82. doi:10.1172/jci31344
85. Strauss, L, Mahmoud, MAA, Weaver, JD, Tijaro-Ovalle, NM, Christofides, A, Wang, Q, et al. Targeted Deletion of PD-1 in Myeloid Cells Induces Antitumor Immunity. Sci Immunol (2020) 5(43):eaay1863. doi:10.1126/sciimmunol.aay1863
86. Dolladille, C, Akroun, J, Morice, PM, Dompmartin, A, Ezine, E, Sassier, M, et al. Cardiovascular Immunotoxicities Associated With Immune Checkpoint Inhibitors: A Safety Meta-Analysis. Eur Heart J (2021) 42(48):4964–77. doi:10.1093/eurheartj/ehab618
87. Calabretta, R, Hoeller, C, Pichler, V, Mitterhauser, M, Karanikas, G, Haug, A, et al. Immune Checkpoint Inhibitor Therapy Induces Inflammatory Activity in Large Arteries. Circulation (2020) 142(24):2396–8. doi:10.1161/circulationaha.120.048708
89. Omori, M, Okuma, Y, Hakozaki, T, and Hosomi, Y. Statins Improve Survival in Patients Previously Treated With Nivolumab for Advanced Non-Small Cell Lung Cancer: An Observational Study. Mol Clin Oncol (2019) 10(1):137–43. doi:10.3892/mco.2018.1765
90. Cantini, L, Pecci, F, Hurkmans, DP, Belderbos, RA, Lanese, A, Copparoni, C, et al. High-Intensity Statins Are Associated With Improved Clinical Activity of PD-1 Inhibitors in Malignant Pleural Mesothelioma and Advanced Non-small Cell Lung Cancer Patients. Eur J Cancer (2021) 144:41–8. doi:10.1016/j.ejca.2020.10.031
91. Buti, S, Bersanelli, M, Perrone, F, Tiseo, M, Tucci, M, Adamo, V, et al. Effect of Concomitant Medications With Immune-Modulatory Properties on the Outcomes of Patients With Advanced Cancer Treated With Immune Checkpoint Inhibitors: Development and Validation of a Novel Prognostic index. Eur J Cancer (2021) 142:18–28. doi:10.1016/j.ejca.2020.09.033
92. Cortellini, A, Tucci, M, Adamo, V, Stucci, LS, Russo, A, Tanda, ET, et al. Integrated Analysis of Concomitant Medications and Oncological Outcomes From PD-1/pd-L1 Checkpoint Inhibitors in Clinical Practice. J ImmunoTherapy Cancer (2020) 8(2):e001361. doi:10.1136/jitc-2020-001361
93. Zhang, Y, Chen, H, Chen, S, Li, Z, Chen, J, and Li, W. The Effect of Concomitant Use of Statins, NSAIDs, Low-Dose Aspirin, Metformin and Beta-Blockers on Outcomes in Patients Receiving Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Oncoimmunology (2021) 10(1):1957605. doi:10.1080/2162402x.2021.1957605
94. Svaton, M, Zemanova, M, Zemanova, P, Kultan, J, Fischer, O, Skrickova, J, et al. Impact of Concomitant Medication Administered at the Time of Initiation of Nivolumab Therapy on Outcome in Non-small Cell Lung Cancer. Anticancer Res (2020) 40(4):2209–17. doi:10.21873/anticanres.14182
95. Failing, JJ, Finnes, HD, Kottschade, LA, Allred, JB, and Markovic, SN. Effects of Commonly Used Chronic Medications on the Outcomes of Ipilimumab Therapy in Patients With Metastatic Melanoma. Melanoma Res (2016) 26(6):609–15. doi:10.1097/cmr.0000000000000299
96. Liu, X, Bao, X, Hu, M, Chang, H, Jiao, M, Cheng, J, et al. Inhibition of PCSK9 Potentiates Immune Checkpoint Therapy for Cancer. Nature (2020) 588(7839):693–8. doi:10.1038/s41586-020-2911-7
97. Ball, S, Ghosh, RK, Wongsaengsak, S, Bandyopadhyay, D, Ghosh, GC, Aronow, WS, et al. Cardiovascular Toxicities of Immune Checkpoint Inhibitors: JACC Review Topic of the Week. J Am Coll Cardiol (2019) 74(13):1714–27. doi:10.1016/j.jacc.2019.07.079
98. Lyon, AR, Yousaf, N, Battisti, NML, Moslehi, J, and Larkin, J. Immune Checkpoint Inhibitors and Cardiovascular Toxicity. Lancet Oncol (2018) 19(9):e447–e458. doi:10.1016/s1470-2045(18)30457-1
99. Serzan, M, Rapisuwon, S, Krishnan, J, Chang, IC, and Barac, A. Takotsubo Cardiomyopathy Associated With Checkpoint Inhibitor Therapy: Endomyocardial Biopsy Provides Pathological Insights to Dual Diseases. JACC: CardioOncology (2021) 3(2):330–4. doi:10.1016/j.jaccao.2021.02.005
100. Zhang, H, Watanabe, R, Berry, GJ, Vaglio, A, Liao, YJ, Warrington, KJ, et al. Immunoinhibitory Checkpoint Deficiency in Medium and Large Vessel Vasculitis. Proc Natl Acad Sci U S A (2017) 114(6):E970–e979. doi:10.1073/pnas.1616848114
101. Watanabe, R, Zhang, H, Berry, G, Goronzy, JJ, and Weyand, CM. Immune Checkpoint Dysfunction in Large and Medium Vessel Vasculitis. Am J Physiology-Heart Circulatory Physiol (2017) 312(5):H1052–h1059. doi:10.1152/ajpheart.00024.2017
102. Daxini, A, Cronin, K, and Sreih, AG Vasculitis Associated With Immune Checkpoint Inhibitors—A Systematic Review. Clin Rheumatol (2018) 37(9):2579–84. doi:10.1007/s10067-018-4177-0
103. Thuny, F, Naidoo, J, and Neilan, TG Cardiovascular Complications of Immune Checkpoint Inhibitors for Cancer. Eur Heart J (2022) 43(42):4458–68. doi:10.1093/eurheartj/ehac456
104. Wang, TF, and Carrier, M Immune Checkpoint Inhibitors-Associated Thrombosis: Incidence, Risk Factors and Management. Curr Oncol (2023) 30(3):3032–46. doi:10.3390/curroncol30030230
105. Solinas, C, Saba, L, Sganzerla, P, and Petrelli, F. Venous and Arterial Thromboembolic Events With Immune Checkpoint Inhibitors: A Systematic Review. Thromb Res (2020) 196:444–53. doi:10.1016/j.thromres.2020.09.038
Keywords: immune checkpoint inhibitor, myocarditis, pericarditis, ICI rechallenge, glucocorticoids
Citation: Paluri RK, Pulipati Y and Regalla DKR (2023) Immune Checkpoint Inhibitors and Their Cardiovascular Adverse Effects. Oncol. Rev. 17:11456. doi: 10.3389/or.2023.11456
Received: 08 April 2023; Accepted: 25 October 2023;
Published: 17 November 2023.
Edited by:
Sandro Barni, ASST di Bergamo Ovest, ItalyReviewed by:
Alessandro Inno, Ospedale Sacro Cuore Don Calabria, ItalyArjun Khunger, Peacehealth Sacred Heart Medical center at Riverbend, United States
Copyright © 2023 Paluri, Pulipati and Regalla. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dileep Kumar Reddy Regalla, dileepkumar.r.regalla@osfhealthcare.org, regalladileepreddy@gmail.com