
Palliative Care for Cancer Patients in Asia: Challenges and Countermeasures
 Yu Wang
Yu Wang Xinqing Zhang2,
Xinqing Zhang2, - 1Department of Radiation Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
- 2School of Humanities and Social Sciences, Peking Union Medical College, Beijing, China
- 3Division of Prevention and Community Health, National Center for Cardiovascular Disease, National Clinical Research Center of Cardiovascular Disease, State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
With the increasing incidence of cancer worldwide, palliative care has become an effective intervention to relieve cancer patients’ pain and improve their quality of life, although the present development of palliative medicine and hospice care in many Asian countries remains insufficient. To this end, this review comprehensively discussed the main challenges that influence the promotion of palliative medicine, from the perspective of both healthcare professionals and cancer patients. We further proposed and summarized a series of potentially effective countermeasures and solutions, including the shared decision-making modal, multidisciplinary professional cooperation, application of modern science and technology, standardization training for medical workers, personalized palliative treatment regimens, and others, aiming to improve the clinical quality of palliative care practice for cancer patients and promote the development of palliative medicine in Asian regions.
Introduction
In recent years, with the rapid development of Asian economy and medicine, the spectrum of clinical diseases has undergone significant changes. The incidence of parasitic diseases and other infectious diseases in Asia had greatly reduced, while the incidence of malignant diseases is increasing [1–3]. Cancer is the leading cause of global disease burden [4]. The clinical features of cancer include difficulty to cure, rapid progression and higher medical cost. Thus, cancer diseases could bring a huge physical and mental burden to patients and their families [5].
Palliative care, as an important component of people-oriented health services, aims to alleviate severe suffering related to disease and improve the quality of life, and has become an effective intervention widely used in the treatment of cancer [6]. However, the development of palliative care for cancer patients in many Asian regions remains incomplete and inadequate [7, 8]. The awareness and knowledge of palliative medicine and advanced care planning were at low levels even in the diverse Asian groups living in the United States, which raised concerns and demonstrated the urgent need for appropriate education programs on palliative care in Asia [9]. The purpose of this review is to comprehensively explore the specific factors and challenges influencing cancer palliative care in Asian regions and further propose potential countermeasures with clinical practical significance.
The academic term “palliative care” was first used by a Canadian physician named Balfour Mound in 1974, when he incorporated principles from the British hospice movement into acute care hospitals in Canada first and then around the world [10]. Further three main features were developed in palliative care programs: multidimensional assessment and management of severe physical or emotional distress, professional medical care by multiple disciplines, and emphasis on caring not only for the patients but also for their families [11]. Currently, the academic community generally agrees with the definition revised by the World Health Organization (WHO) in 2016—“Palliative care is a crucial part of integrated, people-centred health services and relieving serious health-related suffering” [12]. Therefore, palliative medicine, also known as palliative care, is not only an effective medical intervention, but a comprehensive method to improve the quality of end-stage life, which has become the consensus of most definitions [13]. At the same time, palliative care also has a holistic view and takes various dimensions into account, including physical, mental, social, spiritual and economical condition of patients, which is especially helpful to those terminally ill patients with advanced cancer, experiencing pain and suffering [14, 15].
The promotion of palliative care is a global ethical responsibility. Patients suffering from a variety of conditions, such as cancer, cardiovascular disease, acute organ failure, severe burns, end-stage chronic disease, severe trauma or extremely fragility, and many other acute or chronic diseases, may all benefit from palliative care to manage their symptoms and improve their quality of life. As such, palliative care should to be emphasized and incorporated into all levels of medical practice over time [16]. According to statistics from WHO, it is estimated that globally only 14% of patients who require palliative care can receive it [12]. In order to attain the Sustainable Development Goals and achieve universal health coverage, countries have to strengthen palliative care services and take it as a key part of health systems.
The definition of “Hospice care” is widely identified by the academic community as follows: Hospice care, including psychological and spiritual supports provided by medical professionals and volunteers, helps the dying person achieve peace, comfort and dignity, and mainly focuses on end-of-life patients, as well as their families [17]. Therefore, hospice care refers to the care and nursing services provided by medical staff, social groups and volunteers for critically ill patients and their families, so that all of them can correctly face and accept the terminal stage of the disease and the death [18].
At present, the application of hospice care, especially in patients with advanced cancer, has received special attention, because it can effectively relieve pain and improve quality of life, while comforting their families and relieving their psychosocial burden caused by cancer. When oncologists proactively discuss end-of-life concerns, patients and their family members tend to choose more comfort-focused care aligned with their values and goals [19]. Furthermore, hospice care—a care service that focuses on end-stage patients and their families—is widely encouraged and gradually integrated into comprehensive cancer treatment regimens nowadays, given the additional integration of cancer services with hospice care will help to provide more seamless care for patients and support for family caregivers during their caregiving and after the death of patients [20].
Current Status of Palliative Care in Asia
Due to the particularity of cancer, most patients and their families may first encounter the term “palliative care” under the guidance, explanations, and suggestions from their doctors. Currently, the awareness of palliative care is lower in many Asian developing countries, such as China and India, compared to developed countries in Europe and America. Although the Chinese government has increased its support for palliative care in recent years, owing to the lack of education around hospice care and the influence of the traditional Chinese Confucian concept of “filial piety,” many individuals resist palliative medicine, especially in rural areas [21]. In addition, ethnic minority groups in Asia are less likely to discuss issues involving end-of-life treatment preferences and utilize palliative care or hospice services; language barriers, religion, lower levels of health literacy, and limited access to healthcare services and information may contribute to these disparities [22]. A latest cross-sectional study by Yu et al. [23] identified insufficient knowledge and inappropriate behaviours in breakthrough cancer pain diagnosis, assessments, and management among practitioners providing palliative care in Shanghai, China, highlighting an urgent need to improve the quality of cancer palliative care practice in this region.
Similarly, in Thailand, Wongprom et al. [24] demonstrated the gap between expected care and actual care in grief management and spiritual care, though they have been recognized as essential domains in palliative care practice. Grief and bereavement care were mentioned in the residency curriculum in Thailand, whereas there were contradictions and inconsistency with respect to spiritual care practice [24]. Meanwhile, Prachanukool et al. [25] further suggested the early integration of palliative care and hospice consultation into the clinical management for patients at their end-of-life stages, which reflects the conceptual development and practical improvements on palliative care in Thailand.
Hence, despite the underdeveloped status quo of palliative medicine in multiple Asian countries, palliative and hospice care has been greatly promoted on the account of the rapid progress of Asian medical and health undertakings [26]. For example, the community-based palliative care model has been recently established in Busan city, Korea, based on principles of palliative medicine and characteristics of public health, aiming to develop the medical support system, increase professional personnel capacity, and improve the quality of palliative care in Korea [27]. Likewise, in Japan, providing palliative care is one of the most important health issues, and palliative medicine in Japan has also progressed rapidly, with two major specialized palliative services: palliative care units and hospital palliative care consultation teams [28]. At present, the number of palliative care units in Japan is 215 (involved in 8.4% of all cancer deaths), and there already are approximately 500 hospital palliative care teams [28]. In India, palliative care providers lobbied to gain access to methadone for pain relief and this has finally been achieved in recent years, which also represented a progress of palliative care, to some extent [29]. Palliative care activists in India counted on numerous strengths, including the various national and state government initiatives that have been introduced recognizing the importance of palliative care. Moreover, National Network of Palliative Care is one of the largest community-driven palliative care programs in the world, with branches in more than ten states in India to date [29, 30].
Although Singapore has established itself as a leading multifaceted medical hub and continues to pursue excellence in palliative care, Loh et al. [31] observed insufficient integration of allied health and rehabilitation services, passive engagement of community partners, lack of specialized skill sets and knowledge in cancer supportive and survivorship care in Singapore. Additionally, a retrospective review of 683 patients died without intensive care unit admission in a Singaporean hospital, which evaluated the prevalence of do-not-resuscitate (DNR) orders, revealed a lack of commitment by doctors on orders for both DNR and to limit life-sustaining therapies [32]. Even in the Asian developed country, Singapore, there were infrequent discussions with patients on end-of-life clinical decisions and excessive burdensome interventions for the dying [32]. Hence, the appropriate and high-quality palliative care practice is still somewhat lacking in Asian developed countries, and should be attached more importance in the future. The status quo of palliative care in the different Asian countries is summarized in Table 1.
TABLE 1
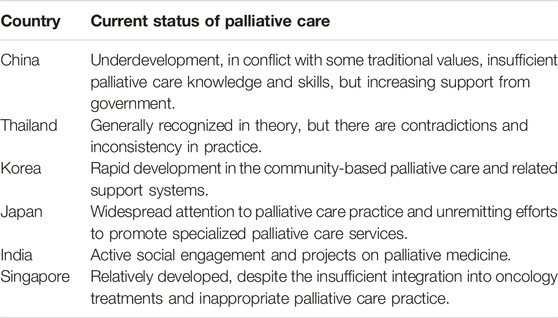
TABLE 1. The current situation of palliative care in several Asian countries.
Challenges of Palliative Care Practice in Asian Regions
Conflicts of Traditional Values in Asians
When scholars explored the obstacles in developing palliative medicine practice, they found that the individual conflicts of traditional values might be the main factor in Asian regions [32]. For instance, in ancient Chinese culture, the death or illness was deemed unlucky, and people would be as much as possible to avoid discussions regarding “death”. Besides, the traditional Chinese Confucian concept of “filial piety” may also mislead patients to choose inappropriate radical treatment at an inappropriate time, and thus let them become rejective to palliative medicine [21, 33]. These negative attitudes and avoidance to end-of-life topic could against the education and promotion of palliative care, to a large extent. Therefore, an attitudinal shift regarding the pain and illness is in urgent need through extensive and inspiring public educational activities in India and many other Asian developing countries [29]. In India, studies indicated that patients’ experiences of spirituality are determined by the specifically Indian traditional context, which also gives rise to particular ethical issues and challenges in palliative care [34].
At the same time, the alienation and the war metaphor of disease have deepened the dualism of medical outcome evaluation, probably leading individuals to mistake hospice care for a “failed and abandoned” choice [35]. The misperception of palliative medicine as giving up could leave undesirable impression on patients and their families in some Asian regions, negatively influence the public acceptance, deepen their fear of illness, and result in adverse impacts.
Limited Availability of Medical Recourse
Recent studies have showed that community health services remain inadequate in China, especially with respect to home-based palliative care, albeit the majority of cancer patients have a preference of home death [36, 37]. As such, limited resources of palliative care would inevitably affect the choice and acceptance of patients and their families. In addition to China, home hospice is inconsistently available in many other Asian countries, and very few of them have enough palliative care specialists to meet their current workforce needs, let alone meet anticipated future needs [38]. For instance, although opioids are accepted as essential for cancer pain treatment globally, the accessibility and availability of this medicine are very limited in India as in various parts of the developing world [29].
Of note, on 15 April 2006, the establishment of China Life Care Association (CLCA) marked the arrival of the spring of hospice care in China. The comprehensive oncology care service of Hong Kong University-Shenzhen Hospital (HKU-SZH), which was established in 2012 as a new model of publicly funded healthcare in mainland China, achieved a satisfactory level of end-of-life care in patients with advanced cancer [39]. Since previous studies indicated inappropriate and inadequate palliative care practice even in Singapore [31, 40], in addition to intensified public education, completing supportive policy, and increasing palliative care facilities in developing countries, public availability to high-quality palliative care services should be emphasized in Asian developed countries when it comes to promoting palliative medicine.
Clinical Expertise of Physicians
Nowadays the clinical medical staff remain the major practitioner of palliative care worldwide [41]. Thus, ideally district hospitals should train doctors, nurses, pharmacists, and social workers in primary palliative care centres. In addition, a well-defined curriculum and educational program is also needed to ensure uniform training for palliative care providers, when the palliative consultation especially for cancer patients has significantly increased in recent years [42]. When physicians are going to adopt palliative care towards patients with advanced cancer or other end-stage conditions, their professional knowledge, clinical skills and positive attitude are necessary. In daily clinical oncology practice, it is impossible to provide a safe, reliable and high-quality palliative care planning without expertise. In consequences, clinicians need to accumulate the practical experience and professional knowledge of palliative care, constantly popular the public education and promote the general understanding of palliative care in Asian regions. Moreover, drawing on the useful experience from Western developed countries, it is important to emphasize palliative care in clinical practice guidelines, along with regulation, training and certification of care providers, to ensure reliable access to palliative care in Asia.
Family Support and Socioeconomic Background
In recent years, with the economic development and life quality improvement, great changes have taken place in many Asian countries. For example, the incidences of infectious and parasitic diseases have significantly reduced, and incidences of malignant tumours are growing [1, 2]. Cancer diseases are difficult to cure, causing huge economic burden and social pressure, and aggravating the physical and mental pain of patients. At the same time, palliative and hospice care for cancer patients require not only sufficient medical resources from doctors, but also abundant human resources input from patient families. Studies indicated that family caregivers provided substantial care for patients with advanced cancer, while suffering from hidden morbidity and unmet needs [43]. As a direct consequence of assuming the caregiver role, cancer family caregivers play an important role in the palliative care, but also are at increased risk for physical and mental pressure in hospice and bereavement phases [44, 45]. Therefore, in addition to treatment willingness of cancer patients, the understanding and supports of their families and social networks, as well as their socioeconomic background, both are crucial factors influencing the decisions on palliative care.
Countermeasures to Promote Palliative Care in Asia
Shared Decision-Making Model
In order to help cancer patients and their families make appropriate decisions with respect to palliative care, medical staff, patients and their families need to openly discuss the objective condition, true treatment willingness of patients, their medical demands and specific treatment options, so as to further prepare for the doctor-patient cooperation. Meanwhile, the nursing staff, as health educators, palliative caregivers and medical information conveyer, should also be actively involved in the medical decision-making work, aiming to provide high-quality palliative care. Obviously, healthcare professionals are trained to be expert in planning treatment regimens, yet patients are more aware of their lifestyle, environment, financial situation and how much they can rely on home care resources [46]. As a result, the shared decision-making model is becoming more and more important in modern medicine. On the basis of effective communication and cooperation between doctors and patients, the shared decision-making model for palliative care will achieve the optimal clinical results.
More importantly, medical workers should fully respect and understand the choices of patients. The appropriate end-of-life care measures are based on the willing acceptance and approval of patients and their families [47]. Only in this way can medical interventions achieve maximum clinical benefits. Given the substantial development of co-decision in clinical practice, especially in the field of cancer treatment, this beneficial healthcare model also should be applied and promoted in palliative medicine.
Professional Multidisciplinary Cooperation
Palliative treatment and hospice care for patients with advanced cancer have been concerned by more and more clinicians, humanistic ethics scholars and social activists. In 2014, World Health Assembly (WHA) adopted a landmark resolution calling on all member states to take palliative care as part of comprehensive cancer treatment, and to give it sufficient attention and practical application in cancer multidisciplinary treatment [48, 49].
At present, the multidisciplinary team involvement is commonplace in many treatment settings across the world. Teamwork is also perceived by many experts as an indispensable functionality of palliative care teams [50]. Among the palliative care models carried out in Asian regions, most of them were as follows: 1) Professional palliative care institutions and program: the community ward based on multidisciplinary program, with medical care and entertainment facilities (such as Indian National Program in Palliative Care, The Busan Community-based Palliative Care Project in Korea) [29, 51]; 2) Palliative wards in general hospitals: using hospital resources to provide medical service, nursing and supportive care for terminally ill patients, based on multidisciplinary cooperation (such as the department of palliative and hospice care of West China Fourth Hospital, department of palliative medicine of Tsukuba Medical Center Hospital in Japan, and department of palliative medicine of Tan Tock Seng Hospital in Singapore) [52–54]; 3) Specialized palliative medical units established in cancer hospitals: providing palliative care services for cancer patients (such as the palliative care centre of Peking University Cancer Hospital in China) [55].
To sum up, although the specific presentation model of palliative medicine varies, the successful healthcare services are always on the basis of the multidisciplinary team cooperation. Therefore, it is essential to attach importance to multidisciplinary professional medical team, in order to provide more comprehensive palliative treatment with high quality in Asian regions.
Clinical Utility of Modern Technology
Despite the high potential to improve the quality of life, palliative care services face significant obstacles to their use in some Asian regions, probably due to limitations of technology and economics in some Asian developing countries [56]. Nowadays, with artificial intelligence (AI), machine learning, robotic surgery and the Internet big data, more and more clinical work can be replaced by the modern high technology. These modern technologies are now applied to various clinical medical practice [57]. In the field of palliative medicine, the combination of modern scientific technologies with the careful care and professional expertise from medical staff may further facilitate the development of palliative care in Asia.
As a consequence, in order to advance palliative medicine and optimize palliative care services utilization in Asian regions, the combination of technology and humanity, as well as the subjective and objective application of medical progress brought by high-technology improvements, both are of great value. Additionally, a shift in public perspective, concerning the use of modern technology in palliative care managements, also should be encouraged. Because based on the modern scientific technology, clinicians are more likely to provide improved high-quality palliative care for cancer patients and their families, and accordingly better help them face the end-of-life diseases and death.
Personalized Palliative Treatment
Given different physical and psychosocial condition of every cancer patient, the personalized palliative care treatment regimen should be adopted in Asian countries with corresponding medical conditions. To this end, emphasizing accurate diagnoses, appropriate therapeutic regimens and corresponding adjustment according to the real-time situation is of great value in developing palliative care level in Asian regions [58].
Currently, personalized medicine based on tumour characteristics is transforming the management of cancer. Personalized oncology is evidence-based, individualized medicine that delivers the right care to the right cancer patient at the right time and thus results in measurable improvements in outcomes and further reductions on medical costs. In the future, palliative care givers should focus more on every individual patient, using the optimal and personalized treatment regimen to manage pain, other uncomfortable symptoms and negative emotions. More importantly, in the light of different values, beliefs, social and economic background of patients and their families, caregivers should attach importance to meet their subjective needs and guide them to correctly face the cancer disease. To provide patients all-round positive palliative care, medical staff ought to change the key point from “disease-oriented” to “patient-centred.” Only on this basis can we enhance the quality of palliative care for cancer patients, which is conducive to the progress and development of palliative care practice in Asian regions.
Others
Lastly, there were also some other potential measures and strategies to foster the development of palliative care in Asian regions, such as developing standardized structures for palliative care practice in the community or regional palliative care projects, proposing professional palliative care models suitable for cancer patients, establishing objective methods to measure the quality of palliative care at a national level, and introducing more evidence-based hospice care and palliative medicine to the public and the policymakers [28]. Furthermore, sufficient and appropriate supportive strategies are particularly conducive to patients with advance cancer, such as anticipating, preventing and treating suffering throughout the continuum of illness, and effectively addressing symptom distress. Besides, eliciting value-based goals of cancer care, respecting the DNR wishes of patients and hold to the commitment, allowing withholding or withdrawal of life sustaining measures, and attaching more importance to bereavement support are all vital to cancer patients and their families [31].
Discussion
Taken together, current development of palliative care in most Asian countries remains insufficient, probably due to some traditional value conflicts, limited availability of palliative care, inadequate training in palliative medicine for medical personnel, lack of family supports and finite socioeconomic background of patients. In order to improve the quality of hospice care for cancer patients and their families in Asia and promote the development of palliative care, countermeasures such as shared decision-making, multidisciplinary cooperation, standardized palliative care training for medical workers, clinical application of modern scientific techniques, personalized palliative treatments, and other potential strategies should be adopted. As such, palliative care practice for cancer patients will be improved in Asia.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This work was supported by the Special Research Fund for Central Universities, Peking Union Medical College (No. 3332023133 and No. 3332023026).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors appreciate Xuefeng Wang for his guidance and assistance.
References
1. Siegel, RL, Miller, KD, Fuchs, HE, and Jemal, A. Cancer Statistics, 2021. CA: A Cancer J Clinicians (2021) 71(1):7–33. doi:10.3322/caac.21654
2. Jiang, Y, Dou, X, Yan, C, Wan, L, Liu, H, Li, M, et al. Epidemiological Characteristics and Trends of Notifiable Infectious Diseases in China From 1986 to 2016. J Glob Health (2020) 10(2):020803. doi:10.7189/jogh.10.020803
3. Zheng, R, Zhang, S, Zeng, H, Wang, S, Sun, K, Chen, R, et al. Cancer incidence and mortality in China, 2016. Journal of the National Cancer Center (2022) 2(1):1–9. doi:10.1016/j.jncc.2022.02.002
4. Jemal, A, Bray, F, Center, MM, Ferlay, J, Ward, E, and Forman, D. Global Cancer Statistics. CA: A Cancer J clinicians (2011) 61(2):69–90. doi:10.3322/caac.20107
5. de Martel, C, Georges, D, Bray, F, Ferlay, J, and Clifford, GM. Global Burden of Cancer Attributable to Infections in 2018: A Worldwide Incidence Analysis. Lancet Glob Health (2020) 8(2):e180–e190. doi:10.1016/s2214-109x(19)30488-7
6. Ferrell, BR, Temel, JS, Temin, S, Alesi, ER, Balboni, TA, Basch, EM, et al. Integration of Palliative Care Into Standard Oncology Care: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol (2017) 35(1):96–112. doi:10.1200/jco.2016.70.1474
7. Dosani, N, Bhargava, R, Arya, A, Pang, C, Tut, P, Sharma, A, et al. Perceptions of Palliative Care in a South Asian Community: Findings From an Observational Study. BMC Palliat Care (2020) 19(1):141. doi:10.1186/s12904-020-00646-6
8. Brown, E, Franklin, A, and Coad, J. A Concept Analysis in Relation to the Cultural Competency of the Palliative Care Workforce in Meeting the Needs of Young People From South Asian Cultures. Palliat Support Care (2018) 16(2):220–7. doi:10.1017/s1478951517000207
9. Shen, JJ, Dingley, C, Yoo, JW, Rathi, S, Kim, SK, Kang, HT, et al. Sociocultural Factors Associated With Awareness of Palliative Care and Advanced Care Planning Among Asian Populations. Ethn Dis (2020) 30(3):459–68. doi:10.18865/ed.30.3.459
10. Saga, Y, Enokido, M, Iwata, Y, and Ogawa, A. Transitions in Palliative Care: Conceptual Diversification and the Integration of Palliative Care Into Standard Oncology Care. Chin Clin Oncol (2018) 7(3):32. doi:10.21037/cco.2018.06.02
11. Lutz, S. The History of Hospice and Palliative Care. Curr Probl Cancer (2011) 35(6):304–9. doi:10.1016/j.currproblcancer.2011.10.004
12. WHO. Palliative Care (2021). Available at: https://www.who.int/health-topics/palliative-care (Accessed October 23, 2021).
13. Radbruch, L, De Lima, L, Knaul, F, Wenk, R, Ali, Z, Bhatnaghar, S, et al. Redefining Palliative Care-A New Consensus-Based Definition. J pain symptom Manag (2020) 60(4):754–64. doi:10.1016/j.jpainsymman.2020.04.027
14. Heydari, H, Hojjat-Assari, S, Almasian, M, and Pirjani, P. Exploring Health Care Providers' Perceptions About Home-Based Palliative Care in Terminally Ill Cancer Patients. BMC Palliat Care (2019) 18(1):66. doi:10.1186/s12904-019-0452-3
15. Wang, T, Molassiotis, A, Chung, BPM, and Tan, JY. Unmet Care Needs of Advanced Cancer Patients and Their Informal Caregivers: A Systematic Review. BMC Palliat Care (2018) 17(1):96. doi:10.1186/s12904-018-0346-9
16. Verkissen, MN, Hjermstad, MJ, Van Belle, S, Kaasa, S, Deliens, L, and Pardon, K. Quality of Life and Symptom Intensity Over Time in People With Cancer Receiving Palliative Care: Results From the International European Palliative Care Cancer Symptom Study. PloS one (2019) 14(10):e0222988. doi:10.1371/journal.pone.0222988
17. McCann, BA. Hospice Care in the United States: The Struggle for Definition and Survival. J Palliat Care (1988) 4(1-2):16–8. doi:10.1177/0825859788004001-206
18. Shepperd, S, Gonçalves-Bradley, DC, Straus, SE, and Wee, B. Hospital at Home: Home-Based End-Of-Life Care. Cochrane database Syst Rev (2016) 2(2):Cd009231. doi:10.1002/14651858.CD009231.pub2
19. Buss, MK, Rock, LK, and McCarthy, EP. Understanding Palliative Care and Hospice: A Review for Primary Care Providers. Mayo Clinic Proc (2017) 92(2):280–6. doi:10.1016/j.mayocp.2016.11.007
20. Currow, DC, Agar, MR, and Phillips, JL. Role of Hospice Care at the End of Life for People With Cancer. J Clin Oncol (2020) 38(9):937–43. doi:10.1200/jco.18.02235
21. Ling, M, Wang, X, Ma, Y, and Long, Y. A Review of the Current State of Hospice Care in China. Curr Oncol Rep (2020) 22(10):99. doi:10.1007/s11912-020-00959-y
22. Mayeda, DP, and Ward, KT. Methods for Overcoming Barriers in Palliative Care for Ethnic/Racial Minorities: A Systematic Review. Palliat Support Care (2019) 17(6):697–706. doi:10.1017/s1478951519000403
23. Yu, Y, Zhang, P, Chen, D, and Jiang, SF. Knowledge and Practice of the Management of Breakthrough Cancer Pain Among General Practitioners Providing Palliative Care in Shanghai, China: A Cross-Sectional Survey. BMJ Open (2023) 13(9):e073670. doi:10.1136/bmjopen-2023-073670
24. Wongprom, I, and Chaithanasarn, A. A Survey of Palliative Care Domains and the Palliative Care Provision Confidence of Thai Family Practitioners. BMC Palliat Care (2023) 22(1):147. doi:10.1186/s12904-023-01272-8
25. Prachanukool, T, George, N, Bowman, J, Ito, K, and Ouchi, K. Best Practices in End of Life and Palliative Care in the Emergency Department. Clin Geriatr Med (2023) 39(4):575–97. doi:10.1016/j.cger.2023.05.011
26. Malloy, P, Takenouchi, S, Kim, HS, Lu, Y, and Ferrell, B. Providing Palliative Care Education: Showcasing Efforts of Asian Nurses. Asia-Pacific J Oncol Nurs (2018) 5(1):15–20. doi:10.4103/apjon.apjon_55_17
27. Kim, SN, Choi, SO, Shin, SH, Ryu, JS, and Baik, JW. Development of a Community-Based Palliative Care Model for Advance Cancer Patients in Public Health Centers in Busan, Korea. Cancer Res Treat (2017) 49(3):559–68. doi:10.4143/crt.2016.276
28. Morita, T, and Kizawa, Y. Palliative Care in Japan: A Review Focusing on Care Delivery System. Curr Opin Support Palliat Care (2013) 7(2):207–15. doi:10.1097/SPC.0b013e3283612241
29. Viswanath, V, Palat, G, Chary, S, and Broderick, A. Challenges of Using Methadone in the Indian Pain and Palliative Care Practice. Indian J Palliat Care (2018) 24(1):S30–s35. doi:10.4103/ijpc.Ijpc_168_17
30. Kumar, SK. Kerala, India: A Regional Community-Based Palliative Care Model. J pain symptom Manag (2007) 33(5):623–7. doi:10.1016/j.jpainsymman.2007.02.005
31. Phua, J, Kee, AC, Tan, A, Mukhopadhyay, A, See, KC, Aung, NW, et al. End-of-Life Care in the General Wards of a Singaporean Hospital: An Asian Perspective. J Palliat Med (2011) 14(12):1296–301. doi:10.1089/jpm.2011.0215
32. Huang, V, and Fiocco, AJ. Measuring Perceived Receipt of Filial Piety Among Chinese Middle-Aged and Older Adults. J cross-cultural Gerontol (2020) 35(2):195–208. doi:10.1007/s10823-019-09391-7
33. Zhou, J, Guo, Q, and Xu, R. Reciprocal Filial Piety Facilitates Academic Success via Autonomy: Generalizing Findings in Chinese Society to a Global Context. Front Psychol (2020) 11:69. doi:10.3389/fpsyg.2020.00069
34. Gielen, J, Bhatnagar, S, and Chaturvedi, SK. Spirituality as an Ethical Challenge in Indian Palliative Care: A Systematic Review. Palliat Support Care (2016) 14(5):561–82. doi:10.1017/s147895151500125x
35. Institute of Medicine Forum on Microbial. The National Academies Collection: Reports Funded by National Institutes of Health. Washington: National Academy of Sciences (2006).
36. Cai, J, Zhang, L, Guerriere, D, Fan, H, and Coyte, PC. Where Do Cancer Patients in Receipt of Home-Based Palliative Care Prefer to Die and What Are the Determinants of a Preference for a Home Death? Int J Environ Res Public Health (2020) 18(1):235. doi:10.3390/ijerph18010235
37. Cai, J, Zhang, L, Guerriere, D, and Coyte, PC. Congruence Between Preferred and Actual Place of Death for Those in Receipt of Home-Based Palliative Care. J Palliat Med (2020) 23(11):1460–7. doi:10.1089/jpm.2019.0582
38. Hawley, P. Barriers to Access to Palliative Care. Palliat Care Res Treat (2017) 10:117822421668888. doi:10.1177/1178224216688887
39. Li, JS, Lam, TC, Jing, HM, Chen, X, Cao, MY, Huang, C, et al. Quality of End-Of-Life Care of Advanced Cancer Patients in Mainland China-A Retrospective Cohort of 441 Hospital-Death in a Public Funded Comprehensive Hospital. Ann Palliat Med (2020) 9(6):4514–20. doi:10.21037/apm-19-268
40. Loh, KW, Ng, T, Choo, SP, Saw, HM, Mahendran, R, Tan, C, et al. Cancer Supportive and Survivorship Care in Singapore: Current Challenges and Future Outlook. J Glob Oncol (2018) 4:1–8. doi:10.1200/jgo.17.00117
41. Bateman, RM, Sharpe, MD, Jagger, JE, Ellis, CG, Solé-Violán, J, López-Rodríguez, M, et al. 36th International Symposium on Intensive Care and Emergency Medicine: Brussels, Belgium. 15-18 March 2016. Crit Care (2016) 20(Suppl. 2):94. doi:10.1186/s13054-016-1208-6
42. Patel, AA, Walling, AM, Ricks-Oddie, J, May, FP, Saab, S, and Wenger, N. Palliative Care and Health Care Utilization for Patients With End-Stage Liver Disease at the End of Life. Clinical Gastroenterology and Hepatology: The Official Clinical Practice. Clin Gastroenterol Hepatol (2017) 15(10):1612–9.e4. doi:10.1016/j.cgh.2017.01.030
43. Alam, S, Hannon, B, and Zimmermann, C. Palliative Care for Family Caregivers. J Clin Oncol (2020) 38(9):926–36. doi:10.1200/jco.19.00018
44. Williams, AL, and McCorkle, R. Cancer Family Caregivers During the Palliative, Hospice, and Bereavement Phases: A Review of the Descriptive Psychosocial Literature. Palliat Support Care (2011) 9(3):315–25. doi:10.1017/s1478951511000265
45. Guldin, MB, Vedsted, P, Zachariae, R, Olesen, F, and Jensen, AB. Complicated Grief and Need for Professional Support in Family Caregivers of Cancer Patients in Palliative Care: A Longitudinal Cohort Study. Support Care Cancer (2012) 20(8):1679–85. doi:10.1007/s00520-011-1260-3
46. Horgan, D, Bolanos, N, Mastris, K, Mendao, L, and Malats, N. Health Literacy: Read All About It. Biomed hub (2017) 2(1):1–4. doi:10.1159/000481129
47. Hjelmfors, L, Strömberg, A, Friedrichsen, M, Sandgren, A, Mårtensson, J, and Jaarsma, T. Using Co-Design to Develop an Intervention to Improve Communication About the Heart Failure Trajectory and End-Of-Life Care. BMC Palliat Care (2018) 17(1):85. doi:10.1186/s12904-018-0340-2
48. Carrasco, JM, Inbadas, H, Whitelaw, A, and Clark, D. Early Impact of the 2014 World Health Assembly Resolution on Palliative Care: A Qualitative Study Using Semistructured Interviews With Key Experts. J Palliat Med (2021) 24(1):103–6. doi:10.1089/jpm.2019.0384
49. van der Rijt, T, and Pang Pangestu, T. Governance Within the World Health Assembly: A 13-Year Analysis of WHO Member States' Contribution to Global Health Governance. Health policy (2015) 119(3):395–404. doi:10.1016/j.healthpol.2014.12.008
50. Fernando, G, and Hughes, S. Team Approaches in Palliative Care: A Review of the Literature. Int J Palliat Nurs (2019) 25(9):444–51. doi:10.12968/ijpn.2019.25.9.444
51. Choi, SO, Kim, SN, Shin, SH, Ryu, JS, Baik, JW, Kim, JR, et al. Evaluation of Outcomes of the Busan Community-Based Palliative Care Project in Korea. Asian Nurs Res (2018) 12(4):286–92. doi:10.1016/j.anr.2018.11.001
52. Li, J, Davis, MP, and Gamier, P. Palliative Medicine: Barriers and Developments in Mainland China. Curr Oncol Rep (2011) 13(4):290–4. doi:10.1007/s11912-011-0169-9
53. Kinoshita, S, Miyashita, M, Morita, T, Sato, K, Shoji, A, Chiba, Y, et al. Japanese Bereaved Family Members' Perspectives of Palliative Care Units and Palliative Care: J-HOPE Study Results. Am J Hosp Palliat Medicine® (2016) 33(5):425–30. doi:10.1177/1049909115578385
54. Cheng, SY, Lin, CP, Chan, HY, Martina, D, Mori, M, Kim, SH, et al. Advance Care Planning in Asian Culture. Jpn J Clin Oncol (2020) 50(9):976–89. doi:10.1093/jjco/hyaa131
55. Zhong, X, Song, Y, Dennis, C, Slovensky, DJ, Wei, LY, Chen, J, et al. Patient Safety Culture in Peking University Cancer Hospital in China: Baseline Assessment and Comparative Analysis for Quality Improvement. BMC Health Serv Res (2019) 19(1):1008. doi:10.1186/s12913-019-4837-z
56. Bennardi, M, Diviani, N, Gamondi, C, Stüssi, G, Saletti, P, Cinesi, I, et al. Palliative Care Utilization in Oncology and Hemato-Oncology: A Systematic Review of Cognitive Barriers and Facilitators From the Perspective of Healthcare Professionals, Adult Patients, and Their Families. BMC Palliat Care (2020) 19(1):47. doi:10.1186/s12904-020-00556-7
57. Mekov, E, Miravitlles, M, and Petkov, R. Artificial Intelligence and Machine Learning in Respiratory Medicine. Expert Rev Respir Med (2020) 14(6):559–64. doi:10.1080/17476348.2020.1743181
58. Wang, Y, Zhang, T, Huang, Y, Li, W, Zhao, J, Yang, Y, et al. Real-World Safety and Efficacy of Consolidation Durvalumab After Chemoradiation Therapy for Stage III Non-small Cell Lung Cancer: A Systematic Review and Meta-analysis. Int J Radiat Oncol Biol Phys (2022) 112(5):1154–1164. doi:10.1016/j.ijrobp.2021.12.150
Keywords: palliative care, hospice care, cancer, personalized medicine, review
Citation: Wang Y, Zhang X, Huang Y and Ma X (2024) Palliative Care for Cancer Patients in Asia: Challenges and Countermeasures. Oncol. Rev. 17:11866. doi: 10.3389/or.2023.11866
Received: 27 July 2023; Accepted: 29 November 2023;
Published: 16 January 2024.
Edited by:
Deepa Kushwaha, Rare Genomics Institute, United StatesReviewed by:
Zhizheng Zhuo, Capital Medical University, ChinaMengya Li, Chinese Academy of Medical Sciences and Peking Union Medical College, China
Copyright © 2024 Wang, Zhang, Huang and Ma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiangyu Ma, mxyccmu@sina.com