 Dahabo Adi Galgalo1,2,3*
Dahabo Adi Galgalo1,2,3* Kiptulon Evans Kasmai1
Kiptulon Evans Kasmai1 Kálmán András Kovács3,4,5
Kálmán András Kovács3,4,5 Viktória Prémusz1,3,5,6†
Viktória Prémusz1,3,5,6† Ákos Várnagy3,4,5†
Ákos Várnagy3,4,5†- 1Doctoral School of Health Science, Faculty of Health Science, University of Pécs, Pécs, Hungary
- 2Department of Health, Marsabit, Kenya
- 3National Laboratory on Human Reproduction, University of Pécs, Pécs, Hungary
- 4Department of Obstetrics and Gynaecology, Medical School, University of Pécs, Pécs, Hungary
- 5HUN-REN-PTE Human Reproduction Scientific Research Group, Pécs, Hungary
- 6Institute of Physiotherapy and Sport Sciences, Faculty of Health Sciences, University of Pécs, Pécs, Hungary
Introduction: All pregnant women are encouraged to visit Antenatal Care (ANC) during pregnancy to ensure their wellbeing and that of their unborn baby. World Health Organization (WHO) recommends that all pregnant women attend antenatal clinics for care at least eight times during pregnancy. During antenatal care a series of essential tests are done for pregnant women, both clinical examination and laboratory screenings to detect potential issues which will guide clinicians on management. This study aims to investigate the clinical examination and laboratory screening profile results of pastoralist pregnant women and its associated factors during their first ANC visit in Marsabit County, Kenya.
Methods: A cross-sectional study was conducted among pregnant women who attended Integrated Maternal Mobile (IMMH) outreach clinics for ANC in 10 mobile pastoralist communities. Data were collected on demographic information, clinical examination information, and laboratory profile screening outcomes. Frequency and percentages were used to describe the categorical variables and means and standard deviations were used to describe the continuous variables. Bivariate and multivariate analysis was conducted using IBM SPPS 27.0 following STROBE guidelines. The level of significance was set at p < 0.05.
Results: Data (N = 237) were extracted, the mean age was 26.62 ± 5.371, of which the majority were in the age group of 20–29, 212 (89.5%) were married 180 (75.9%) and multigravida, 27 (11.4%) visited ANC and 121 (51.1%) traveling more than 15 km to seek healthcare services. The mean weight was 55.56 ± 9.019 kg, mean blood pressure systolic was 118.94 ± 19.95 mmHg, and diastolic was 73.87 ± 13.46 mmHg. Out of all specimens processed and tested, 135 (57%) were anaemic with Hgb <11.5 g/dL), 6 (2.5%) had malaria, 8 (3.4%) were hepatitis B positive, and 21 (8.9%) showed intestinal infection. Those women who are illiterate displayed a 12-fold higher likelihood of becoming anaemic during pregnancy (OR 11.50, 95% CI: 2.47–53.47), and those who didn’t attend ANC also have a 5-fold higher likelihood of being anaemic (OR 5.43, 95% CI: 2.52–11.70).
Conclusion: Anaemia, hepatitis B, syphilis, malaria parasites, intestinal parasites, and urinary tract infections were observed among the study participants. Integrated outreach programs with laboratory screening and health education should be enhanced, and women within pastoralist communities should be empowered through health education.
Introduction
Maternal, New-born, and Child Health (MNCH) indicator improvement is one of the Sustainable Development Goals (SDGs) agenda, where the main aim is to reduce the global burden of maternal, new-born, and child mortality (Knbs, 2023; World Health Organization, 2018). Despite international efforts and progress, maternal deaths are still high, of which almost 800 pregnant women die annually from pregnancy-related complications worldwide, and over 90% of those deaths are experienced in Asia and Sub-Saharan African regions (Khalil et al., 2023). Maternal mortality rates in Kenya have decreased from 362/100,000 live births in 2014 to 355/100,00 live births in 2022, which is still high compared to global incidence rates (Knbs, 2023). In most developing countries the direct causes of maternal mortality include; postpartum hemorrhage, hypertensive disorders, infections, obstructed labour, unsafe abortion, and ruptured uterus (Bhandari and Dangal, 2014), which contribute to almost 78% of all deaths while remaining are caused by indirect causes like anaemia, diabetes, malaria, tuberculosis and Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS) (Girum and Wasie, 2017). Most causes of these deaths are conditions that can be prevented if proper screening is given during antenatal and postnatal care (Say et al., 2014).
The 2016 WHO Antenatal Care model aims to provide at least eight ANC contacts to all pregnant women. The primary contact occurs in the first trimester, the second and third contacts in the second trimester, and the remaining five contacts in the third trimester (World Health Organization, 2016). The first-trimester contact is very important for assessing the women’s health by identifying risk factors and establishing a baseline for subsequent care (Tunçalp et al., 2017). Some of the antenatal profiles that should be done during the first trimester as indicated in the Mother and Child Health booklet by the Ministry of Health (MOH)-Kenya (Mudany et al., 2015) include; hemoglobin level, blood grouping, and rhesus factors, urinalysis, random blood sugar (RBS), syphilis, hepatitis B, HIV counselling and testing, and Mycobacteria Tuberculosis (TBC) screening.
Despite efforts made by the Kenyan government to enhance MNCH in North Eastern counties, Marsabit County still has low MNCH indicators (Keats et al., 2017). The county has four major sub-counties namely: North Horr, Moyale, Saku, and Laisamis, The proportion of pastoralists within the county is 81%, with the majority residing in Moyale Sub-County. It is the largest, most arid area, with the majority of the population being pastoralists, and the least developed county in Kenya. According to the 2022 Kenya Demographic Health Survey (KDHIS 2022), Marsabit County had 67% ANC coverage, 59.3% health facility deliveries, 41% postpartum check-ups, and 62% of women aged 15–49 have no formal education (Knbs, 2023). At the county level, most of the health facilities that provide ANC services concentrate in the county and sub-county hospitals, of which only a few provide ANC services. Dispensaries and clinics have no laboratories but provide ANC consultation (Muga et al., 2005). WHO recommended that all pregnant women should be referred to a laboratory for the complete set of ANC screening tests during the first ANC visit (Abalos et al., 2016). During pregnancy, a woman’s body undergoes significant changes and monitoring is very important for early intervention (Azab et al., 2020). Marsabit County, being one of the vast counties in Kenya, has very few medical laboratories for testing, and also almost 80% of the residents are pastoralists; therefore, few pregnant women have access to healthcare facilities for testing.
Clinical examination and laboratory screening during antenatal visits are considered timely to prevent, identify, and correct the abnormalities that might affect the mother and foetus. The findings guide the clinicians in treating existing diseases or others that may occur during pregnancy leading to early intervention and treatment (Anversa et al., 2012; Habte et al., 2024). Inadequate care during pregnancy breaks a critical link in the continuum of care and affects both women and the foetus (Ahmed and Mohamed, 2018). Some of the risk factors like anaemia, high blood pressure, diabetes, undiagnosed infections, and other pre-existing health conditions frequently complicate pregnancy (Gupton et al., 2001). No research has been done in Marsabit County to understand pastoralist pregnant women’s clinical examination and laboratory antenatal screening. Therefore, this cross-sectional study aims to describe the clinical and laboratory presentation of pastoralist pregnant women during the first antenatal visit, which includes the prevalence of hypertension, urinary tract infection, anaemia, syphilis, intestinal parasite infection, hepatitis infections, and any demographic-associated factors.
Materials and methods
The study population was pastoralist pregnant women attending the Integrated Maternal Mobile Health (IMMH) outreach clinic in Moyale Sub-County, Marsabit County, Kenya. The IMMH project provides health services to pregnant pastoralist women through a health outreach program. The study was done in ten mobile/pastoralist communities, which include, Chirach, El-raya, Er-wede, Funandimo, Laqi, Mansile Water Point, Qalaliwe, Qilta, Tesso, and Yaballo Godha.
Study design
A cross-sectional study of pregnant women attending IMMH outreach clinics was conducted from November to December 2021.
Data collection and definitions
Data on demographic, clinical, and laboratory information were extracted from the main Integrated Maternal Mobile Health (IMMH) register during the outreach program. Demographic information includes the village, age, marital status, literacy level, marital practice (monogamy or polygamy), possession of a mobile phone, distance from the health facility, antenatal clinic visit, gravidae, and clinical information such as weight and blood pressure were collected. Laboratory information includes haemoglobin level, blood grouping, hepatitis B surface antigen (HBsAg) test, malaria test, syphilis test, urine for urinalysis, and stool for eggs (ova) and cysts.
Sample collection and analysis
Haemoglobin estimation was done using a portable haemoglobin estimation instrument HemoCue RHB 301 analyzer manufactured by A Danaher company (250 S. Kraemer Blvd./Mail Stop BI.SW.11 Brea, CA 92821, United States), it is calibrated against the haemoglobin cyanide (HiCN) methods, the international reference method for the determination of the haemoglobin concentration in blood. Venous blood was collected into a micro cuvette and a drop of it was used within 50 s of withdrawal for haemoglobin estimation. Anemia in the study was defined as a haemoglobin level below <11.5 g/dL, it was further categorized into, Normal (Hgb>11.5 g/dL), Moderate (Hgb 7.0 g/dL–11.5 g/dL) and severe anemia (Hgb <7 g/dL). Later haemoglobin level was dichotomized into <11.5 g/dL as anaemia (Knbs, 2023) and >=11.5 g/dL as normal haemoglobin (World Health Organization, 2018).
Blood pressures were measured using an automatic blood pressure (BP) analyser. This was done by wrapping the cuff around the upper arm, approximately one inch above the elbow, and the machine was turned on. The machine automatically inflates the cuff to a pressure above the expected systolic pressure, then gradually deflates. The machine detects the Korotkoff sounds as the pressure decreases and displays the systolic and diastolic pressures on its screen. Hypertension was defined as a systolic blood pressure >=140 mmHg and/or a diastolic blood pressure ≥90 mmHg.
Malaria testing was done using Rapid Diagnostic Tests (RDTs) manufactured by Determine™ Abbott Company (Lake County, Illinois United States) which detect specific antigens derived from malaria parasites, this was done by placing a drop of blood into a sample pad on the RDT test card. The test card contains specific reagents that react with malaria antigens, the result was displayed on the pad and read after 20 min. When two red lines appear on the test card it’s an indication that malaria parasite was present and, therefore was reported as positive (Knbs, 2023) and when one line appears, recorded as negative (World Health Organization, 2018).
Hepatitis B and Syphilis were performed with the OnSiteR rapid test kit manufactured by CTK Biotech Inc (Poway, CA, United States), which applies a lateral flow chromatographic immunoassay for the qualitative detection of hepatitis B and treponema pallidum surface antigen and antibody in whole blood. Hepatitis B and Syphilis status were reported as positive when two red lines appeared on the testing strip and negative when only one line appeared. Later, it was coded as Positive (Knbs, 2023), and Negative (World Health Organization, 2018).
Urine for urinalysis and stool for ova and cyst were microscopically examined. Women are asked to bring a stool sample in a stool container; the preparation is done by mixing saline water with the sample, and then a small sample is placed on a glass slide and examined for parasites; the result is categorized into ova and cyst seen, which is coded as (Knbs, 2023) or no ova and cyst seen as (World Health Organization, 2018). Women were encouraged to collect morning urine samples and bring them to the laboratory; the sample was put into a centrifuge; this machine separates the liquid urine from any solid components, such as blood cells, mineral crystals, or microorganisms. The deposit from the centrifuged sample was put on a microscope slide, and then the coverslips on the top of the drop were examined; the findings were later categorized into normal (Knbs, 2023) or abnormal (World Health Organization, 2018); it’s abnormal if the finding includes numerous white blood cells (WBC) > 20 cells/HPF and normal urine if very few WBC were seen per High Power Field (HPF).
The blood grouping was done by placing three drops of blood on the slide, and then three different reagents, which include antibodies A, B, and Rh antibodies were added to each drop; the content was mixed well and checked for the presence of agglutination then reported as per ABO and Rh blood grouping system. A small sample of blood was also used to test blood sugar level by placing a drop of blood onto the test strips, then placing the strip into the Accu-CheckR Glucometer manufactured by (Roche S.A. Quimica e Industrial Rawson in Argentina) after a few seconds, the readings appeared; the result was collected as a continuous variable and later was categorized into normal <7.6 mmol/L (Knbs, 2023), and high >7.6 mmol/L (World Health Organization, 2018).
Statistical analysis
This cross-sectional study was conducted, and data was reported by Strengthening the Reporting of Observation Studies in Epidemiology (STROBE) guidelines (Vandenbroucke et al., 2007). A descriptive study was done, and all categorical variables were described with frequencies and percentages, while continuous variables were described with means and standard deviations. Bivariate analysis was performed using chi-square tests to identify associations between demographic characteristics and laboratory outcomes and also to select relevant variables for the multivariate analysis. Multivariate logistic regression was conducted, and predictive factors were chosen by fitting a logistic regression model using a forward selection procedure. All independent variables that show significant value was introduced in the final prediction model and analysed according to their categories in multivariate logistic regression analysis with enter methods. Before data analysis, the questionnaire was cleaned and coded, and then double data entry verification was applied using Epi Data version 3.1. All analyses were conducted using IBM SPSS version 28.0 (SPSS Inc., Chicago, IL, United States). A p-value less than 0.05 was considered statistically significant.
Results
Sample characteristics
A total of 237 pregnant women from ten mobile pastoralist communities participated in this study. Their mean age was 26.62 ± 5.371, of which the majority were in the age group of 20–29, 212 (89.5%) were married, and 180 (75.9%) were multigravida. The mean weight was 55.56 ± 9.019 (kg), and the mean blood pressure systolic was 118.94 ± 19.95 mmHg, and diastolic was 73.87 ± 13.46 mmHg. The illiteracy level among this population is very high, with 222 (93.7%) of pregnant women who can’t read and write. Approximately 66 (28%) of women are in a polygamous marriage, and 27 (11.4%) possess mobile phones; the proportion of women who had at least visited an antenatal clinic was only 27 (11.4%), and 121 (51.1%) walk more than 15 km to seek healthcare services Table 1.
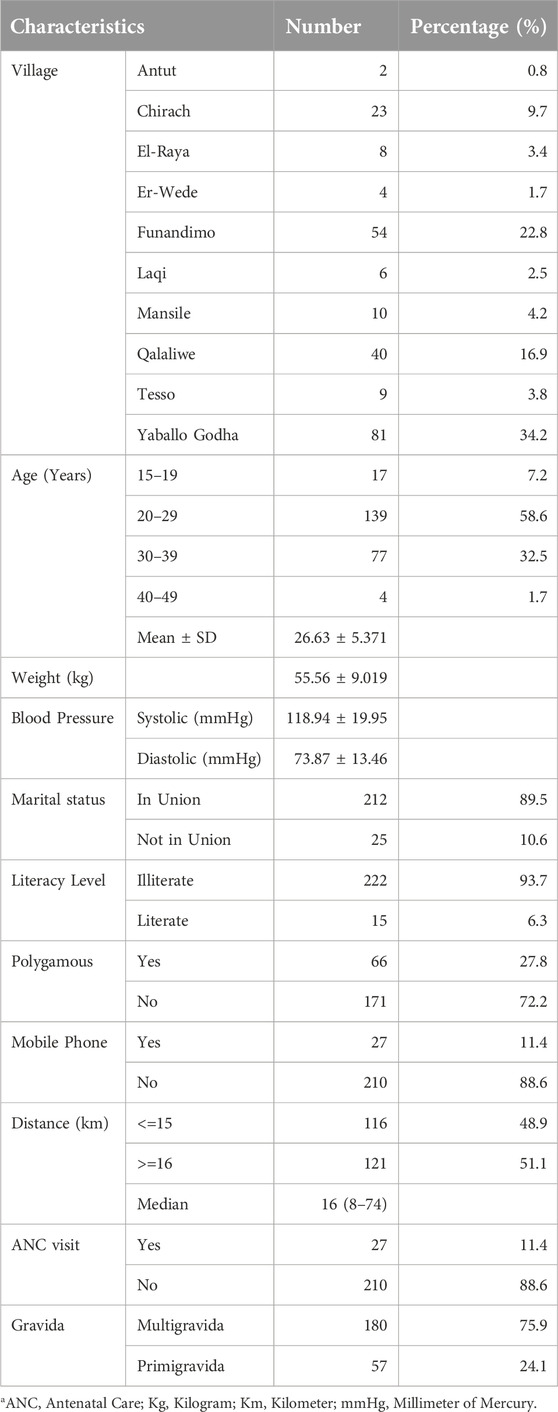
Table 1. Social-demographic information of study participants in Moyale sub-county of Marsabit County, Kenya (N = 237).
Antenatal laboratory screening results
Samples were collected from all 237 participants; out of all samples processed and tested, 135 (57%) had anaemia (haemoglobin level below 11.5 g/dL), 6 (2.5%) were malaria positive, 8 (3.4%) were Hepatitis positive, and 21 (8.9%) showed intestinal infection. The majority of pregnant women, 106 (44.7%), were blood group O Rh positive, and 38 (16.5%) had gestational diabetes mellitus (Table 2).
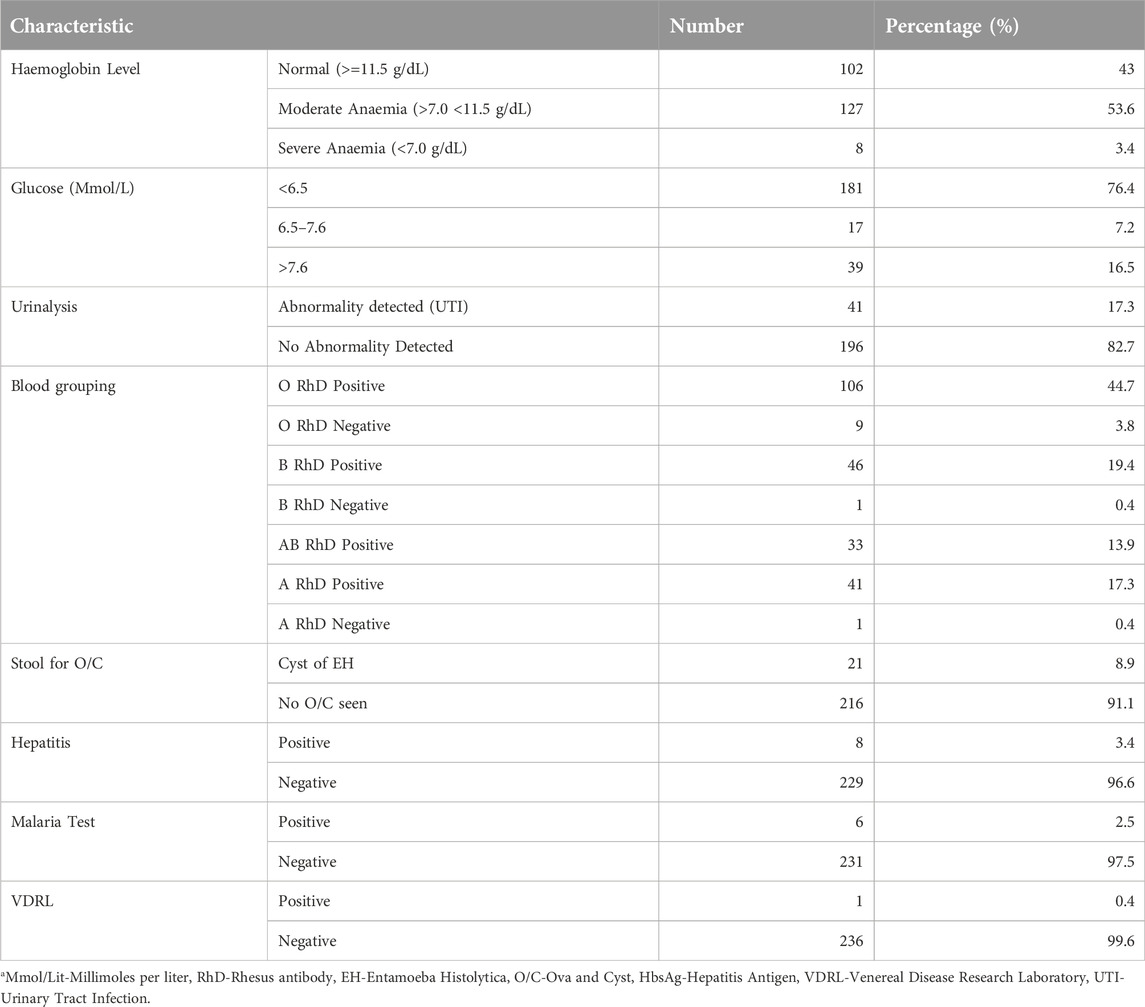
Table 2. Antenatal Laboratory profile results of pastoralist pregnant women who attended the Integrated Maternal Mobile Health Clinic in Marsabit County, Kenya (N = 237).
Bivariate analysis
As per Table 3, the bivariate analysis revealed a significant association between several health variables and laboratory outcomes, that is, haemoglobin level (indicative of anaemia), blood sugar level (linked to hyperglycaemia), Urinalysis results (related to urinary tract infection), and stool for ova and cysts (indicating intestinal worms).
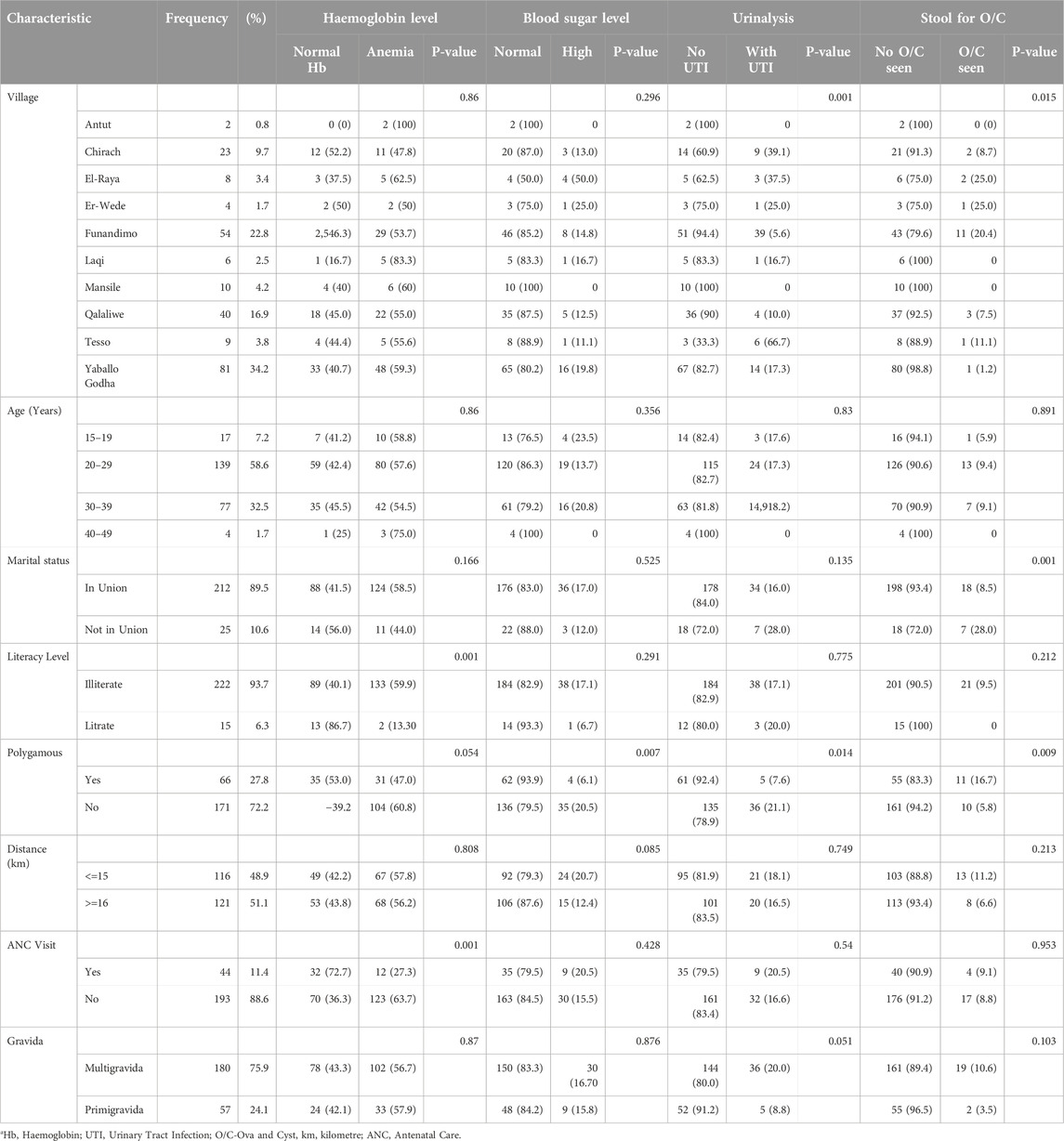
Table 3. Bivariate analysis of antenatal laboratory profile results of pastoralist pregnant women who attended the IMMH outreach in Marsabit County, Kenya.
There was a significant association between the village of residence and the presence of UTI and intestinal infections, with a p-value of 0.001 and 0.015, respectively. In Tesso village, 66.0% of women reported UTIs while both El-Raya and Er-Wede villages showed a 25% incidence of intestinal infections, Women who are not in the union have a significantly higher prevalence of e intestinal worms (n = 7, 28%) compared to women in the union p = 0.001. However, no significance associations were found between union status and anaemia, hypertension, or urinary tract infection. Illiteracy is strongly linked to anaemia, with (n = 133, 59.9%) of uneducated women being affected p = 0.001.
Monogamous marriages correlate with higher rates of anaemia (n = 104, 60.8%), p = 0.054, hypertension, (n = 35, 20.5%) p = 0.007, urinary tract infection (n = 36, 21.1%) p = 0.014, compared to women in a polygamous marriage, but women in polygamous marriages are significantly associated with intestinal worms (n = 11, 16.7%) p = 0.009, compared to women in monogamous marriage.
Pregnant women with multiple pregnancies (multigravida) are more likely to have urinary tract infection (n = 36, 20%), p = 0.051, compared to primigravida.
Women who didn’t attend the antenatal clinic for the duration of their pregnancy were significantly associated with anaemia p = 0.001, (n = 123, 63.7%) compared to women who attended the antenatal clinic during the present pregnancy.
Variables such as age and distance to health facilities did not indicate any significant correlations with haemoglobin level, blood pressure level, urinary tract infections, and intestinal worms.
Multivariable analysis
The results of the multivariate analysis are presented in Tables 4, 5. Indicate that several variables previously identified as significant in bivariate analysis also demonstrate significance in the multivariable analysis. Notably, factors like literacy level and previous antenatal visits for the present pregnancy remained significant for haemoglobin level (anaemia), being monogamous and multigravida remained significant for urinary tract infection, and last but not least being married and having a mobile phone remained significant.
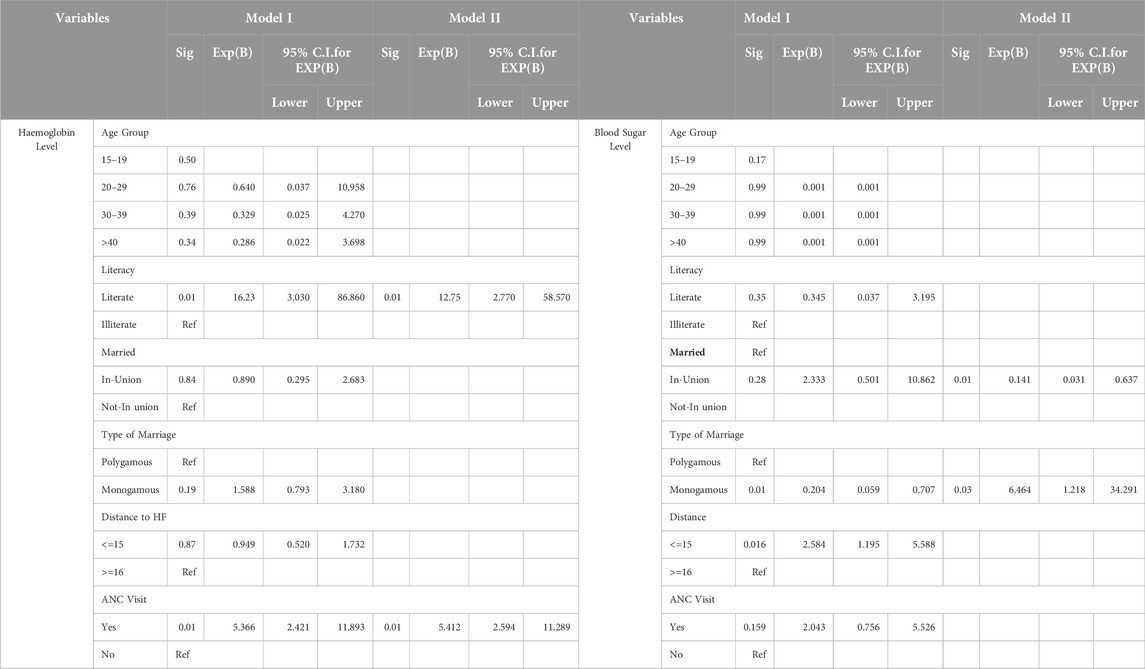
Table 4. Logistic regression of Heamoglobin and Blood sugar level results of pastoralist pregnant women by socio-demographic information.
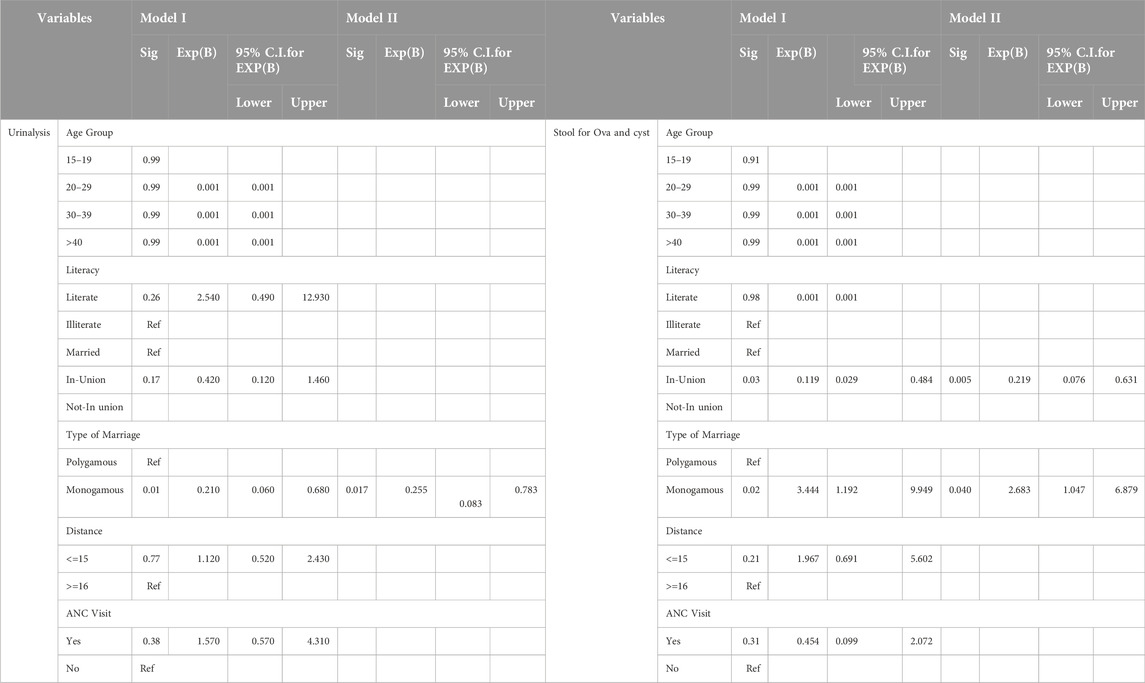
Table 5. Logistic regression of Urinalysis and stool analysis of pastoralist pregnant women by socio-demographic information.
Those women who are illiterate displayed a 12-fold higher likelihood of becoming anaemic during pregnancy (OR 12.75, 95% CI: 2.77–58.57), compared to literate women and those who didn’t attend antenatal clinic also have a 5-fold higher likelihood of being anaemic (OR 5.49, 95% CI: 2.59–11.39), compared to those who didn’t attend antenatal clinic.
Women who are married and live far from health facilities are twice as likely to have hyperglycaemia (OR 2.58, 95% CI: 1.19–5.59).
Pregnant women who are multigravida and practice monogamy show a reduced likelihood of having urinary tract infections (OR 0.33, 95% CI: 0.120–0.916), (OR 0.210, 95% CI: 0.075–0.587), and (OR 1.06, 95% CI: 0.932–1.206), respectively, although some significance is noted for being polygamous and at certain gravida.
Pregnant women who are living in a specific village, at a distance from health facilities, and having co-wives or mobile phones exhibit varying likelihoods of having intestinal parasites, (OR 1.165, 95% CI: 0.952–1.426), (OR 2.14, 95% CI: 0.763–6.006), (OR 1.19, 95% CI: 0.395–3.572) and (OR 4.44, 95% CI: 1.440–13.714) respectively.
Discussion
Clinical examination and laboratory screening are critical when it comes to the management of pregnant women during pregnancy, the findings will guide the clinician to identify any pregnancy-related complications and to put prevention measurements in advance (Bohn and Adeli, 2022). Some of the laboratory screenings that are recommended to be done for all pregnant women are, malaria test, Human Immunodeficiency Virus (HIV), hepatitis virus, syphilis, diabetes, and haemoglobin level (Mudany et al., 2015), but all these depend on the region where women are coming from (World Health Organization, 2018). This study explores the clinical examination and the laboratory antenatal screening outcome of pastoralist pregnant women who attended the IMMH outreach clinic for antenatal care from 10 selected pastoralist communities. The main findings of this research showed that the majority of the participants walk long distances to health facilities, are illiterate, have low attendance of antenatal care and a higher percentage are anaemic. The analysis revealed that illiteracy significantly increases the risk of anaemia during pregnancy. In addition, laboratory outcomes showed some conditions like hyperglycemia, UTI, and intestinal infestation among pregnant women. Overall, these findings illustrated that literacy, antenatal care attendance, marital status, and access to healthcare facilities intertwine to affect maternal health outcomes. This can be addressed through targeted intervention which can significantly improve pregnancy outcomes and reduce complications associated with anaemia, hyperglycaemia, UTIs, and intestinal parasites.
According to the WHO, each pregnant woman must receive at least eight ANC visits, however, only a few pregnant women have at least visited their first antenatal clinic during pregnancy (Habte et al., 2024). According to our findings, only 27 (11.4%) of women were able to attend to antenatal clinic, this finding is consistent with District Health Information Software 2 (DHIS2, 2017) and Marsabit County reproductive maternal new-born child, and adolescent health scorecard of 2017, which showed that almost 3,206 (80%) of these mothers did not achieve the WHO recommendation and antenatal care coverage is 43% against National coverage of 58% (David, 2022). This study is also consistent with a cross-sectional study conducted in Ethiopia among pastoralist communities which shows that only 156 (20%) of women received the recommended standard ANC (Biza and Mohammed, 2016). The majority, 139 (58.6%) of the women were in the age group of 20–29 years, this finding was similar to the study led by Abok (Abok, 2012) in Turkana County on the determining factors for the utilization of ANC among pastoralist women, of which most of the women were aged between 21 and 29 years, and also other study done in Marsabit county which shows the same result (Galgalo et al., 2024). The finding also was consistent with the mean reproductive age of women in Kenya which is 20–24 years as per (DHIS 2020).
Anaemia is a condition that occurs when there are not enough red blood cells to carry sufficient oxygen throughout the body and, it’s a common condition among pregnant women (Gupta, 2020). Anaemia in expectant women has an adverse pregnancy outcome and it’s a serious public health problem (Ogunbode and Ogunbode, 2021). Some of the adverse pregnancy outcome i.e., miscarriage and preterm birth is associated with anaemia (Shen et al., 2015). Our findings show that almost 57% of pregnant women are anaemic, this study differs from the study done in Kenya led by Seteti, (Siteti et al., 2014), which shows that the prevalence of anemia among pregnant women was 40%, This study was consistent with studies done by Acheampong K. and Pobee RA who find that the prevalence of anemia in pregnancy to be more than 50% and 63% respectively. (Acheampong et al., 2018; Pobee et al., 2021). Detection of anemia can help identify important maternal risk factors, and in this study, there was a significant association between illiteracy level and anemia, with women without any form of education being more likely to be anaemic.
Women who didn’t attend the antenatal clinic for the duration of their pregnancy were significantly associated with anemia compared to women who attended. Due to higher illiteracy levels within the pastoralist community women lack knowledge about proper iron-rich foods which may lead to anemia (Hussein, 2016). Iron and nutritional supplements in an integrated program can be used for the prevention and management of pregnancy-related anemia (Siteti et al., 2014). Different countries have shown different ways to treat anaemia in pregnancy like the use of oral iron, intravenous iron, and direct blood transfusion (Al et al., 2005; Burwick and Govindappagari, 2019; Omotayo et al., 2018), Lack of antenatal care among pastoralist communities may be attributed to higher illiteracy level, which is often correlated with limited access to health information and resources. Illiterate women may not understand the importance of iron-rich diets or the risks of anemia during pregnancy (Rai, 2018).
Parasitic infestation was noted among pregnant mothers in this study, this is the most important determinant of anemia and low hemoglobin level. The educational level of women significantly impacts their likelihood of having intestinal worms, as lower education correlates with higher prevalence rates. Studies indicate that women with no formal education are at greater risk for intestinal parasitic infections, including helminths, due to a lack of awareness about hygiene practices and health information necessary for prevention (Feleke and Jember, 2018; Mutalazimah and Mustikaningrum, 2020; Yesuf et al., 2019). Maternal education has been shown to influence not only the health of children but also the prevalence of conditions like anaemia and intestinal infections (Balaji et al., 2022; Quihui et al., 2006; Al-Hindi et al., 2019).
Screening for hepatitis virus is critical during pregnancy, hepatitis virus is a life-threatening liver disease, caused by hepatitis B and C viruses, and it’s a major public health problem, the common mode of transmission is through perinatal vertical transmission or during early childhood (Biondi et al., 2020). A positive mother has up to 90% likelihood of Mother-To-Child Transmission (MTCT) if no prophylaxis is given (Navabakhsh et al., 2011). According to our study, approximately 8 (3.4%) of pregnant women tested positive for hepatitis B virus this is low compared to another study done in Kenya with pooled hepatitis B virus prevalence estimation of 7.8%. (Makokha et al., 2023). But this is consistent with the studies done in Ethiopia and Tanzania, which showed a prevalence rate of 3% (Tegegne et al., 2014), (Metaferia et al., 2016) (Geffert et al., 2020). Some of the arid counties in Kenya, like Marsabit, West Pokot, and Baringo have witnessed an outbreak of Malaria (Owino, 2018). In Kenya malaria remains a major public health problem with over 70% of the population being at risk of the infection (Kenya, 2016), our study finds a prevalence of 2.5% of malaria among pregnant women. Malaria parasite is among the most common and easily preventable causes of poor birth outcomes in the world, and pregnant women are three times more likely to be affected by severe malaria (Kovacs et al., 2015).
According to this study, women in monogamist marriages were significantly more likely to be anaemic, with high blood pressure, and UTI compared to women in polygamous marriages, Women in monogamous families may face challenges related to nutrition and also have limited access to diverse diets or lack awareness about iron-rich foods, and poor dietary choices can lead to anaemia, on the other hand, high blood pressure (hypertension) could be associated with stress and lifestyle factors, women in monogamous marriage may experience stress related to family responsibilities, financial pressures, or social expectations. This chronic stress can contribute to high blood pressure. On the other hand, women in polygamous marriages shared a proximity within the same household, this shared living space could increase the likelihood of exposure to similar environmental conditions. All the above factors are in line with the lower socioeconomic status of monogamous families (Du and Mace, 2019; Coast, 2006; Needham et al., 2021). The study findings indicated that pregnant women who are multigravida are significantly associated with urinary tract infections compared to primigravida. This suggests that the risk of UTIs during pregnancy may be higher for women who have had multiple pregnancies. This finding suggests that the risk of developing UTIs increases with the number of previous pregnancies (MacLean, 2001). This can also be attributed to the anatomical and physiological changes that occur with each pregnancy, these changes can lead to urinary stasis and increased susceptibility to infections. Due to physiological changes, hormonal fluctuations cause ureteral dilation and can compress the bladder, increasing the likelihood of urinary retention and infection. Present in women who had multiple pregnancies, as their bodies may be more affected by these changes (Graseck et al., 2023; Johnson et al., 2021; Delzell and Lefevre, 2000).
Limitations
This is a cross-sectional study therefore, limitations associated with cross-sectional studies are applied to this study. We were not able to generalize these results to pregnant women in all pastoralist-occupied counties, as the women were recruited from only one sub-county.
Conclusion
Clinical examination and laboratory screening are important in the management of pregnant women during pregnancy. This study provides an important finding that requires an implementation within the pastoralist communities to improve the health outcomes of pregnant women. ANC attendance within this population is very low despite recommendations passed by WHO, this shows that pastoralist women miss all opportunities for early screening and intervention of any pregnancy-complicated conditions. Anaemia, hepatitis B, syphilis, malaria parasites, intestinal parasites, and urinary tract infections were observed among the study participants. Higher illiteracy levels and not attending antenatal clinics during pregnancy were also associated with Aneamia. Therefore, fully integrated outreach programs with clinical examination, laboratory screening, and health education to empower pastoralist pregnant women should be enhanced within this community. The findings of this research can be adapted and implemented in frontier counties in Kenya and other countries occupied by pastoralists to enhance maternal healthcare and improve the outcome.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the AMREF Health Africa ESRC in Kenya (registration certificate: AMREF-ESRC P547/2018), the Marsabit Ministry of Health, and the Sub-County Health Management team. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DG played an important role in the conceptualization and planning of the research, the outline of the analysis plan, the results interpretation, the drafting of the article, and the final approval of the version to be published. KE revised the manuscript for important content and worked on interpretation. AV and VP participated in the revision of the manuscript and contributed to the critical revision of the manuscript and the finalization of the article through intellectual reflection. All authors reviewed the results and approved the final version of the manuscript.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The data collected for this study was funded as part of the Grand Challenge Africa 2017 (Grant Nr. GCA/011/114) Seed grant through the Bill and Melinda Gates Foundation. The costs of the publication were financed by ÚNKP-23-4-II-PTE-2061, the New National Excellence Program of the Ministry of Culture and Innovation, the National Research, Development, and Innovation Fund, and the TKP project. -2021-EGA-10 was implemented with the support of the Hungarian National Research, Development, and Innovation Fund, within the framework of the TKP-2021-EGA support system. The authors declare that the design of the study and the collection, analysis, interpretation, and writing of the manuscript are independent of the funding bodies.
Acknowledgments
We are indebted to the pastoralist mothers from Moyale Sub-County who took part in the study. Special thanks to the data collectors and supervisors for their tremendous effort in collecting quality data from the field. Our special thanks go to the University of Pecs, Department of Health Science, for guidance and support in the publication of this paper, and to the Tempus Public Foundation for providing the Stipendium Hungaricum Scholarship.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Abalos, E., Chamillard, M., Diaz, V., Tuncalp, Ӧ., and Gülmezoglu, A. (2016). Antenatal care for healthy pregnant women: a mapping of interventions from existing guidelines to inform the development of new WHO guidance on antenatal care. BJOG An Int. J. Obstetrics & Gynaecol. 123 (4), 519–528. doi:10.1111/1471-0528.13820
Abok, R. E. (2012). Factors influencing maternity services utilization in loima and Turkana central districts of Turkana county.
Acheampong, K., Appiah, S., Baffour-Awuah, D., and Arhin, Y. S. (2018). Prevalence of anemia among pregnant women attending antenatal clinic of a selected hospital in Accra, Ghana. Int. J. Health Sci. Res. 8 (1), 186–193. doi:10.1155/2019/5834159
Ahmed, N. H., and Mohamed, EAEA (2018). Effect of antenatal care on maternal and neonatal outcomes in women’S health hospital. Mansoura Nurs. J. 5 (3), 123–138. doi:10.21608/mnj.2018.154092
Al, R. A., Unlubilgin, E., Kandemir, O., Yalvac, S., Cakir, L., and Haberal, A. (2005). Intravenous versus oral iron for treatment of anemia in pregnancy: A randomized trial. Obstetrics & Gynecol. 106 (6), 1335–1340. doi:10.1097/01.aog.0000185260.82466.b4
Al-Hindi, A., Redwan, A. A., El-Egla, G. O., Abu Qassem, R. R., and Alshammari, A. (2019). Prevalence of intestinal parasitic infections among university female students, Gaza, Palestine. Avicenna J. Med. 09 (04), 143–147. doi:10.4103/ajm.ajm_8_19
Anversa, E. T. R., Bastos, G. A. N., Nunes, L. N., and Dal Pizzol, T. d. S. (2012). Qualidade do processo da assistência pré-natal: unidades básicas de saúde e unidades de Estratégia Saúde da Família em município no Sul do Brasil. Cad. Saúde Pública 28, 789–800. doi:10.1590/s0102-311x2012000400018
Azab, A. E., Albasha, M. O., Jbireal, J., and El Hemady, S. Y. (2020). Haematological changes during pregnancy: Insight into anaemia, leukocytosis, and thrombocytopenia. East Afr. Sch. J. Med. Sci. 3 (5), 185–192. doi:10.11648/j.ajcem.20140202.14
Balaji, K., Priya, V. V., and Gayathri, R. (2022). Knowledge and awareness on iron deficiency anaemia among women-A questionnaire based survey. JETT 13 (6), 80–93. doi:10.47750/jett.2022.13.06.009
Bhandari, T., and Dangal, G. (2014). Emergency obstetric care: strategy for reducing maternal mortality in developing countries. Nepal J. Obstetrics Gynaecol. 9, 8–16. doi:10.3126/njog.v9i1.11179
Biondi, M. J., Marchand-Austin, A., Cronin, K., Nanwa, N., Ravirajan, V., Mandel, E., et al. (2020). Prenatal hepatitis B screening, and hepatitis B burden among children, in ontario: a descriptive study. Cmaj 192 (43), E1299–E1305. doi:10.1503/cmaj.200290
Biza, N., and Mohammed, H. (2016). Pastoralism and antenatal care service utilization in dubti district, Afar, Ethiopia, 2015: A cross-sectional study. Pastoralism 6, 15–17. doi:10.1186/s13570-016-0062-0
Bohn, M. K., and Adeli, K. (2022). Physiological and metabolic adaptations in pregnancy: Importance of trimester-specific reference intervals to investigate maternal health and complications. Crit. Rev. Clin. Laboratory Sci. 59 (2), 76–92. doi:10.1080/10408363.2021.1978923
Burwick, R., and Govindappagari, S. (2019). Treatment of iron deficiency anemia in pregnancy with intravenous versus oral iron: Systematic review and meta-analysis. Am. J. Perinatology 36 (04), 366–376. doi:10.1055/s-0038-1668555
Coast, E. (2006). Maasai marriage: A comparative study of Kenya and Tanzania. J. Comp. Fam. Stud. 37 (3), 399–419. doi:10.3138/jcfs.37.3.399
David, M. (2022). Determinants of utilization of antenatal care services among post-natal women at Saku sub county, Marsabit county, Kenya.
Delzell, J. E., and Lefevre, M. L. (2000). Urinary tract infections during pregnancy. Am. Fam. Physician 61 (3), 713–721.
Du, J., and Mace, R. (2019). Marriage stability in a pastoralist society. Behav. Ecol. 30 (6), 1567–1574. doi:10.1093/beheco/arz115
Feleke, B. E., and Jember, T. H. (2018). Prevalence of helminthic infections and determinant factors among pregnant women in mecha district, northwest Ethiopia: A cross sectional study. BMC Infect. Dis. 18, 373–376. doi:10.1186/s12879-018-3291-6
Galgalo, D. A., Mokaya, P., Chauhan, S., Kiptulon, E. K., Wami, G. A., Várnagy, Á., et al. (2024). Utilization of maternal health care services among pastoralist communities in Marsabit county, Kenya: A cross-sectional survey. Reprod. Health 21 (1), 126. doi:10.1186/s12978-024-01865-3
Geffert, K., Maponga, T. G., Henerico, S., Preiser, W., Mongella, S., Stich, A., et al. (2020). Prevalence of chronic HBV infection in pregnant woman attending antenatal care in a tertiary hospital in mwanza, Tanzania: A cross-sectional study. BMC Infect. Dis. 20, 1–10. doi:10.1186/s12879-020-05096-2
Girum, T., and Wasie, A. (2017). Correlates of maternal mortality in developing countries: An ecological study in 82 countries. Maternal Health, Neonatol. Perinatology 3, 1–6. doi:10.1186/s40748-017-0059-8
Graseck, A. S., Thompson, J. L., Bryant, A. S., Cahill, A. G., Silverman, N. S., and Turrentine, M. A. (2023). Urinary tract infections in pregnant individuals. Obstet. Gynecol. 142 (2), 435–445.
Gupton, A., Heaman, M., and Cheung, L. W. (2001). Complicated and uncomplicated pregnancies: women’s perception of risk. J. Obstetric, Gynecol. & Neonatal Nurs. 30 (2), 192–201. doi:10.1111/j.1552-6909.2001.tb01535.x
Habte, A., Tamene, A., and Melis, T. (2024). Compliance towards WHO recommendations on antenatal care for a positive pregnancy experience: timeliness and adequacy of antenatal care visit in Sub-Saharan African countries: evidence from the most recent standard Demographic Health Survey data. Plos One 19 (1), e0294981. doi:10.1371/journal.pone.0294981
Hussein, A. M. (2016). Effects of pastoralists communtity on quality education in mandera county-Kenya. IOSR J. Humanit. Soc. Sci. 21 (09), 01–09. doi:10.9790/0837-2109100109
Johnson, C. Y., Rocheleau, C. M., Howley, M. M., Chiu, S. K., Arnold, K. E., Ailes, E. C., et al. (2021). Characteristics of women with urinary tract infection in pregnancy. J. Women's Health 30 (11), 1556–1564. doi:10.1089/jwh.2020.8946
Keats, E. C., Ngugi, A., Macharia, W., Akseer, N., Khaemba, E. N., Bhatti, Z., et al. (2017). Progress and priorities for reproductive, maternal, newborn, and child health in Kenya: A countdown to 2015 country case study. Lancet Glob. Health 5 (8), e782–e795. doi:10.1016/s2214-109x(17)30246-2
Kenya, M. (2016). Kenya malaria indicator survey 2015. Nairobi: Nairobi Natl Malar Control Programme Minist Health.
Khalil, A., Samara, A., O’Brien, P., Coutinho, C. M., Quintana, S. M., and Ladhani, S. N. (2023). A call to action: The global failure to effectively tackle maternal mortality rates. Lancet Glob. Health 11 (8), e1165–e1167. doi:10.1016/s2214-109x(23)00247-4
Kovacs, S. D., Rijken, M. J., and Stergachis, A. (2015). Treating severe malaria in pregnancy: A review of the evidence. Drug Saf. 38, 165–181. doi:10.1007/s40264-014-0261-9
MacLean, A. (2001). Urinary tract infection in pregnancy. Int. J. Antimicrob. Agents 17 (4), 273–277. doi:10.1016/s0924-8579(00)00354-x
Makokha, G. N., Zhang, P., Hayes, C. N., Songok, E., and Chayama, K. (2023). The burden of hepatitis B virus infection in Kenya: a systematic review and meta-analysis. Front. Public Health 11, 986020. doi:10.3389/fpubh.2023.986020
Metaferia, Y., Dessie, W., Ali, I., and Amsalu, A. (2016). Seroprevalence and associated risk factors of hepatitis B virus among pregnant women in southern Ethiopia: A hospital-based cross-sectional study. Epidemiol. Health 38, e2016027. doi:10.4178/epih.e2016027
Mudany, M. A., Sirengo, M., Rutherford, G. W., Mwangi, M., Nganga, L. W., and Gichangi, A. (2015). Enhancing maternal and child health using a combined mother & child health booklet in Kenya. J. Trop. Pediatr. 61 (6), 442–447. doi:10.1093/tropej/fmv055
Muga, R., Kizito, P., Mbayah, M., and Gakuruh, T. (2005). Overview of the health system in Kenya. Demogr. Health Surv., 13–26.
Mutalazimah, M., and Mustikaningrum, L. (2020). Knowledge about intestinal worm infection and helminthiasis in pregnant women. Electron J. Gen. Med. 17 (3), em215–2020. doi:10.29333/ejgm/7876
Navabakhsh, B., Mehrabi, N., Estakhri, A., Mohamadnejad, M., and Poustchi, H. (2011). Hepatitis B virus infection during pregnancy: Transmission and prevention. Middle East J. Dig. Dis. 3 (2), 92–102.
Needham, B. L., Straight, B., Hilton, C. E., Olungah, C. O., and Lin, J. (2021). Family socioeconomic status and child telomere length among the Samburu of Kenya. Soc. Sci. & Med. 283, 114182. doi:10.1016/j.socscimed.2021.114182
Ogunbode, O., and Ogunbode, O. (2021). Anaemia in pregnancy. Contemp. Obstetrics Gynecol. Dev. Ctries., 321–330. doi:10.1007/978-3-030-75385-6_29
Omotayo, M. O., Dickin, K. L., Pelletier, D. L., Martin, S. L., Kung’u, J. K., and Stoltzfus, R. J. (2018). Feasibility of integrating calcium and iron–folate supplementation to prevent preeclampsia and anemia in pregnancy in primary healthcare facilities in Kenya. Maternal & Child Nutr. 14, e12437. doi:10.1111/mcn.12437
Owino, E. A. (2018). Kenya needs cohesive policies and better strategies in its war against malaria in arid and semi arid areas. Int. J. Mosq. Res. 5, 124–126. doi:10.1186/s13071-015-0866-6
Pobee, R. A., Setorglo, J., Klevor, M., and Murray-Kolb, L. E. (2021). The prevalence of anemia and iron deficiency among pregnant Ghanaian women, a longitudinal study. PloS One 16 (3), e0248754. doi:10.1371/journal.pone.0248754
Quihui, L., Valencia, M. E., Crompton, D. W., Phillips, S., Hagan, P., Morales, G., et al. (2006). Role of the employment status and education of mothers in the prevalence of intestinal parasitic infections in Mexican rural schoolchildren. BMC Public Health 6, 225–228. doi:10.1186/1471-2458-6-225
Rai, S. (2018). Prevalence of anemia and associated factors among pregnant women of itahari SUB-metropolitan city.
Say, L., Chou, D., Gemmill, A., Tunçalp, Ö., Moller, A. B., Daniels, J., et al. (2014). Global causes of maternal death: a WHO systematic analysis. Lancet Glob. Health 2 (6), e323–e333. doi:10.1016/s2214-109x(14)70227-x
Shen, P. J., Gong, B., Xu, F. Y., and Luo, Y. (2015). Four trace elements in pregnant women and their relationships with adverse pregnancy outcomes. Eur. Rev. Med. Pharmacol. Sci. 19 (24), 4690–4697.
Siteti, M. C., Namasaka, S. D., Ariya, O. P., Injete, S. D., and Wanyonyi, W. A. (2014). Anaemia in pregnancy: prevalence and possible risk factors in Kakamega County, Kenya. Sci. J. Public Health 2 (3), 216–222. doi:10.11648/j.sjph.20140203.23
Tegegne, D., Desta, K., Tegbaru, B., and Tilahun, T. (2014). Seroprevalence and transmission of hepatitis B virus among delivering women and their new born in selected health facilities, addis ababa, Ethiopia: A cross sectional study. BMC Res. Notes 7 (1), 1–7. doi:10.1186/1756-0500-7-239
Tunçalp, Ӧ., Pena-Rosas, J. P., Lawrie, T., Bucagu, M., Oladapo, O. T., Portela, A., et al. (2017). WHO recommendations on antenatal care for a positive pregnancy experience-going beyond survival. Bjog 124 (6), 860–862. doi:10.1111/1471-0528.14599
Vandenbroucke, J. P., Elm, E. von, Altman, D. G., Gøtzsche, P. C., Mulrow, C. D., Pocock, S. J., et al. (2007). Strengthening the reporting of observational studies in Epidemiology (STROBE): Explanation and elaboration. Ann. Intern Med. 147 (8), W–163. doi:10.7326/0003-4819-147-8-200710160-00010-w1
World Health Organization (2016). WHO recommendations on antenatal care for a positive pregnancy experience. World Health Organization.
World Health Organization (2018). WHO recommendations on antenatal care for a positive pregnancy experience: summary: highlights and key messages from the World Health Organization’s 2016 global recommendations for routine antenatal care. World Health Organization.
Yesuf, D. A., Abdissa, L. T., Gerbi, E. A., and Tola, E. K. (2019). Prevalence of intestinal parasitic infection and associated factors among pregnant women attending antenatal care at public health facilities in Lalo Kile district, Oromia, Western Ethiopia. BMC Res. Notes 12, 735–736. doi:10.1186/s13104-019-4781-3
Keywords: laboratory screening, clinical information, anaemia, antenatal care, pastoralist
Citation: Galgalo DA, Evans Kasmai K, Kovács KA, Prémusz V and Várnagy Á (2024) Clinical and laboratory antenatal profile screening and its associate factors among pastoralist women in Northern Part of Kenya. Pastor. Res. Policy Pract. 14:13311. doi: 10.3389/past.2024.13311
Received: 28 May 2024; Accepted: 29 October 2024;
Published: 15 November 2024.
Edited by:
Carol Kerven, University College London, United KingdomCopyright © 2024 Galgalo, Evans Kasmai, Kovács, Prémusz and Várnagy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dahabo Adi Galgalo, YndxaThwQHB0ZS5odQ==
†These authors have contributed equally to this work and share last authorship