
“A Delicate balance”—Perceptions and Experiences of ICU Physicians and Nurses Regarding Controlled Donation After Circulatory Death. A Qualitative Study
 Matthieu Le Dorze1,2*,
Matthieu Le Dorze1,2*,  Sara Martouzet3, Etienne Cassiani-Ingoni1, France Roussin1, Alexandre Mebazaa1,4, Lucas Morin5 and Nancy Kentish-Barnes6
Sara Martouzet3, Etienne Cassiani-Ingoni1, France Roussin1, Alexandre Mebazaa1,4, Lucas Morin5 and Nancy Kentish-Barnes6- 1AP-HP, Hôpital Lariboisière, Department of Anesthesia and Critical Care Medicine, Paris, France
- 2Université Paris-Saclay, UVSQ, INSERM, CESP, U1018, Villejuif, France
- 3Université de Tours, EA 7505 Éducation, Éthique et Santé, Tours, France
- 4Université de Paris, Inserm, UMRS 942 Mascot, Paris, France
- 5INSERM CIC 1431, University Hospital of Besançon, Besançon, France
- 6AP-HP, Saint Louis University Hospital, Famiréa Research Group, Medical Intensive Care Unit, Paris, France
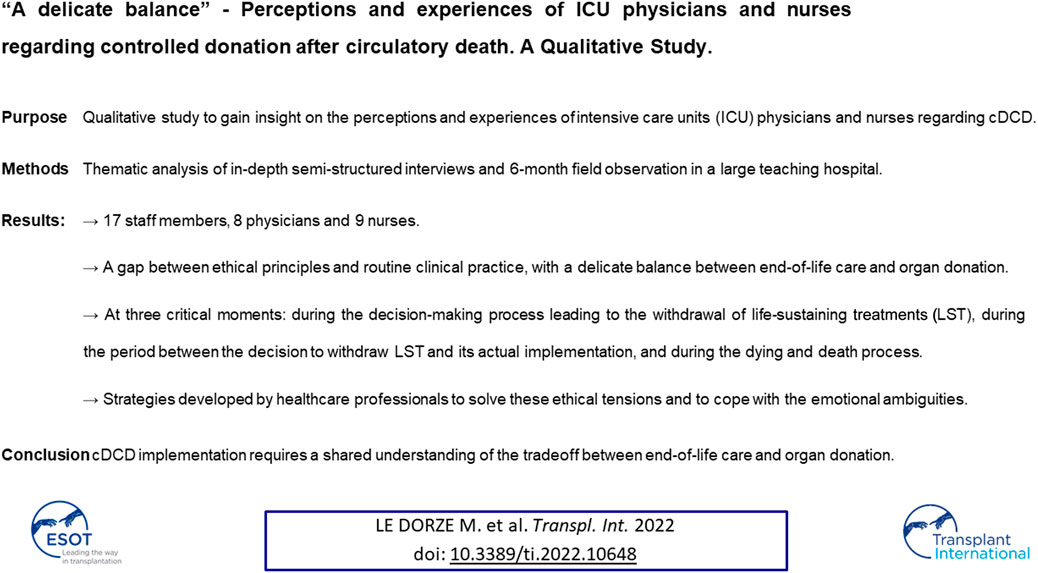
Controlled donation after circulatory death (cDCD) is considered by many as a potential response to the scarcity of donor organs. However, healthcare professionals may feel uncomfortable as end-of-life care and organ donation overlap in cDCD, creating a potential barrier to its development. The aim of this qualitative study was to gain insight on the perceptions and experiences of intensive care units (ICU) physicians and nurses regarding cDCD. We used thematic analysis of in-depth semi-structured interviews and 6-month field observation in a large teaching hospital. 17 staff members (8 physicians and 9 nurses) participated in the study. Analysis showed a gap between ethical principles and routine clinical practice, with a delicate balance between end-of-life care and organ donation. This tension arises at three critical moments: during the decision-making process leading to the withdrawal of life-sustaining treatments (LST), during the period between the decision to withdraw LST and its actual implementation, and during the dying and death process. Our findings shed light on the strategies developed by healthcare professionals to solve these ethical tensions and to cope with the emotional ambiguities. cDCD implementation in routine practice requires a shared understanding of the tradeoff between end-of-life care and organ donation within ICU.
GRAPHICAL ABSTRACT
GRAPHICAL ABSTRACT
Introduction
Controlled donation after circulatory death (cDCD) refers to organ donation from patients whose death is defined using circulatory criteria after the planned withdrawal of life-sustaining treatments (WLST) (1). The scarcity of donor organs and the good transplantation outcomes (2–4) legitimately support the development of this type of donation (5–7) in a context where WLST decisions occur more and more frequently in intensive care units (ICU) worldwide (8–10).
cDCD reshapes end-of-life care by introducing the issue of organ donation before the time of death. Thus, cDCD may potentially affect not only the decision-making process leading to WLST but also other end-of-life care practices (11–14). The French cDCD protocol explicitly states that decision to withdraw LST must be made in the patient’s best interest, independently from any consideration regarding organ donation, and that cDCD must not alter end-of-life care (15). Yet, healthcare professionals can feel particularly uncomfortable when, in practice, end-of-life care and organ donation overlap (16–18). The challenge is not only to identify potential cDCD donors, but also to give healthcare professionals a reassuring ethical framework. Research has shown that physicians and nurses working in ICUs are not always at ease with organ donation after brain death (19).
Developing knowledge on the perceptions and experiences of healthcare professionals regarding cDCD is crucial to improve the quality of the process but remains rarely investigated (16, 17, 18, 20, 21). We conducted a cross-sectional qualitative study to better understand ICU physicians’ and nurses’ experience of cDCD. This will enable to develop interventions to support and guide them throughout this practice, which in turn should not only improve their experience but also the experience of patients’ relatives.
Materials and Methods
To carry out this monocentric qualitative study in an optimal way, we brought together a multidisciplinary research team, which included an ICU physician involved in organ donation (MLD), a graduate student in anthropology student (SM), and a sociologist (NKB).
Objectives
Our objectives were to understand how healthcare professionals perceived WLST decision-making process and how they experienced end-of-life care in this particular context, and finally how their relationship with the patient’s relatives was affected.
Design
In-Depth Interviews
Between May and November 2019, we conducted in-depth interviews with healthcare professionals working in the ICU of a large teaching hospital in central Paris (610 beds overall, including 29 ICU beds). In this ICU, cDCD is implemented according to the ethical and technical requirements of the nationwide protocol, particularly with the systematic use of normothermic regional perfusion (15). The WLST take place preferentially in the ICU, which facilitates the support of relatives by clinicians. When lung retrieval is considered, WLST is exceptionally done in the operating room. In all cases, the ICU team takes care of the patient until death and presence of family members is encouraged if they wish. After the declaration of death, the organ procurement team and a surgical team collaborate on the cannulation and the start of the normothermic regional perfusion.
The semi-structured interview guide was developed a priori by the investigators (Supplementary Table S1). Questions were open-ended, which allowed participants to describe their experience in their own words and to broach specific issues that they considered relevant.
Field Observation
In addition, one investigator (SM) immersed herself full-time in the ICU for a 6-month field observation to better understand the professional culture and the institutional context in which the interviews were conducted (22).
Data Collection
In-Depth Interviews
We used purposeful sampling based on professional status (physicians/nurses) and number of cDCD experiences (23). Participants were recruited through e-mail and personal solicitations. Interviews were conducted individually and in-person by a single investigator (SM) and lasted between 1 and 2 h. All interviews were audio recorded, pseudonymized, and then transcribed verbatim for analysis. Data collection was interrupted when we reached data saturation, namely when no new themes emerged from the interviews (24).
Field Observation
Detailed descriptive notes were taken in the form of a daily research journal. Reflective field notes were also taken. These notes go beyond descriptions to include the researcher’s problems, impressions, analyses, clarifications, syntheses, connections, and other ideas about the research project.
Data Analysis
Primary Data, Interviews
Three researchers (MLD, NKB, and SM) read all the transcripts. Using an inductive approach, they identified initial key themes and concepts that occurred throughout the first three interviews using thematic analysis (25). Then they developed a codebook through an iterative process that ended when the three authors had achieved consensus (26). These authors then coded the same three interviews independently to check for intercoder reliability, after which they convened as a group to discuss potential disagreements and refine the initial themes and categories. Using this consolidated codebook, one researcher (SM) then coded the remaining interviews, adding or modifying codes as necessary given the content of subsequent interviews. Any difficulties or uncertainties were discussed with NKB and MLD during research meetings.
Secondary Data, Observation
Field notes were coded by SM and then discussed and analyzed by NKB and MLD. Field notes allowed us to develop a comprehensive and richer understanding of the interviews and helped confirm thematic analysis of interviews.
Results
A total of 20 staff members were interviewed but due to saturation, a total of 17 were analyzed, including interviews with 8 physicians and 9 nurses (Table 1). No clinician approached refused an interview. Qualitative analysis highlighted the ethical tensions experienced by clinicians at different stages of the process. We identified three key phases in the process, each with specific tensions. These phases and their associated perceived ethical tensions are described below. For each phase, we derived a sample of representative quotes is provided in Tables 2, 3, 4.
TABLE 1

TABLE 1. Characteristics of the study participants.
TABLE 2
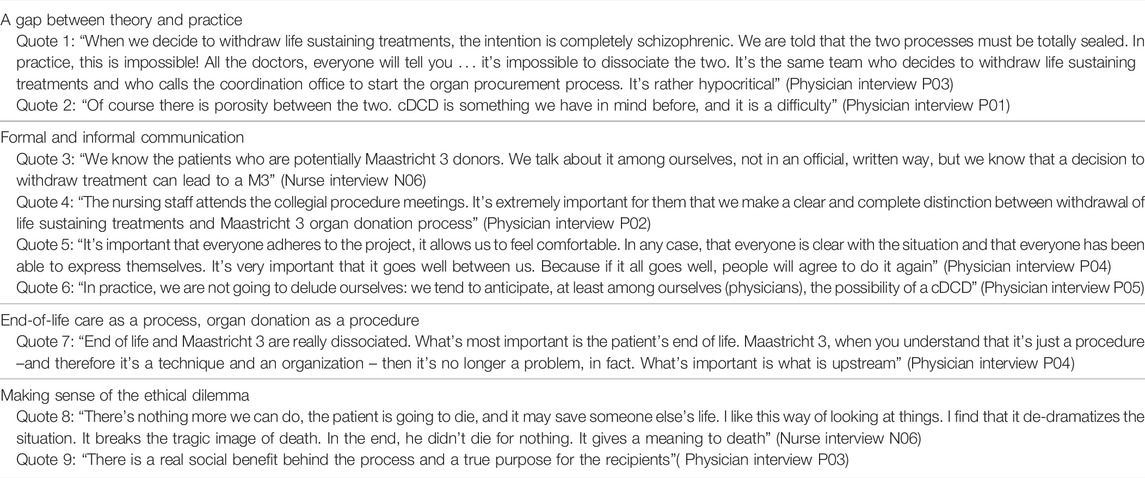
TABLE 2. The decision-making process leading to the withdrawal of life-sustaining treatments in a context of potential organ donation Domains and Quotes.
TABLE 3
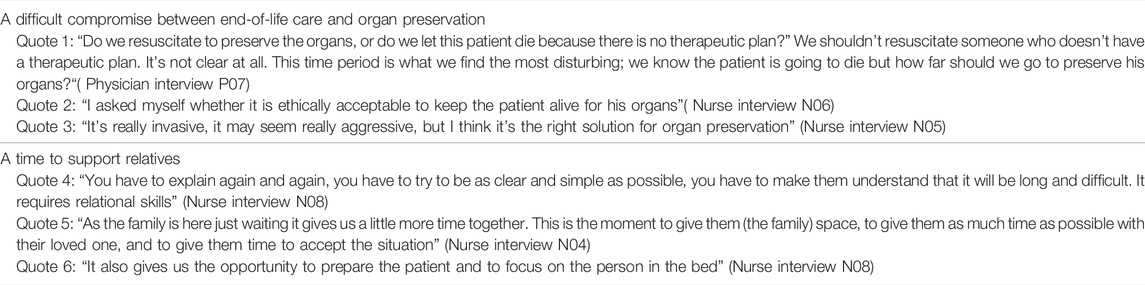
TABLE 3. The period between the decision to withdraw life-sustaining treatment and its actual implementation. Domains and Quotes.
TABLE 4
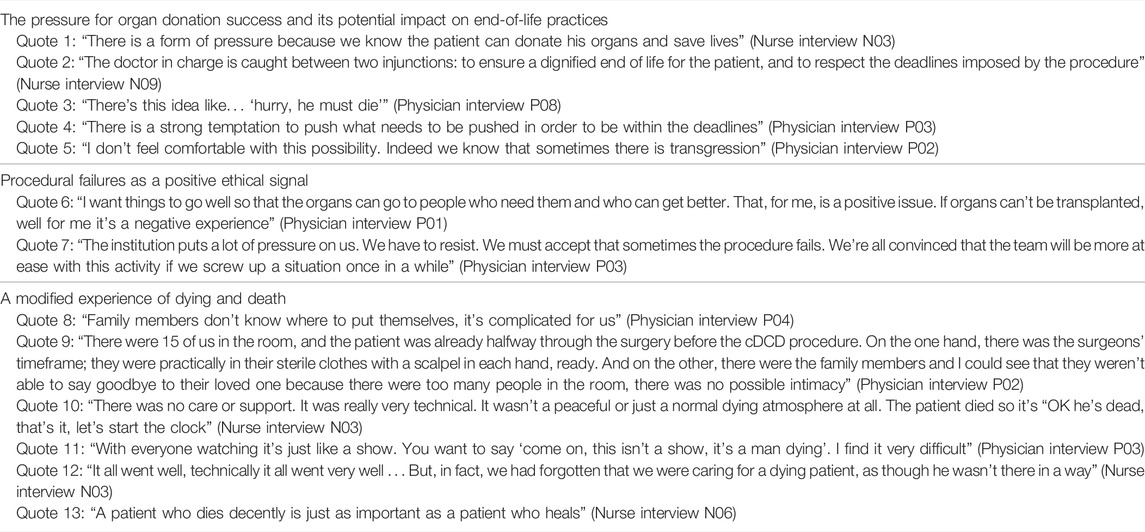
TABLE 4. Dying, death and organ procurement. Domains and Quotes.
Ethical Tensions During the Decision-Making Process Leading to the Withdrawal of Life-Sustaining Treatments in a Context of Potential Organ Donation
A Gap Between Theory and Practice
In theory, the decision to withdraw LST should only be made in the patient’s best interest, must comply with the legal requirements, and should be independent of any subsequent consideration (including organ donation). However, in practice, physicians and nurses expressed their inability to set aside the potentiality of cDCD during the WLST decision-making process (Table 2, quote 1). This gap between theory and practice is experienced as a difficulty (quote 2).
Formal and Informal Communication
One strategy for dealing with this difficulty is to adopt a dual approach combining formal and informal communication (quote 3). Formal communication asserts official recommendations, namely the independence between WLST decision and organ donation possibility. For this purpose, a formal multidisciplinary meeting is organized by the medical team to explicitly reaffirm the priority of the patient’s best interest over the potentiality of organ donation. Field observation revealed that physicians set the scene in order to show to the other ICU staff members that organ donation has not been considered and that attention is focused solely on the WLST decision (quote 4). Physicians explained how, during the meeting, this dissociation between the WLST decision and the possibility of subsequent organ donation helps healthcare professionals to understand and accept the decision (quote 5). They also believed that it legitimated the WLST decision by removing doubt concerning a possible conflict of interest. In contrast, backstage informal communication allowed to consider organ donation as a possibility during the WLST decision-making process (quote 6).
End-of-Life Care as a Process, Organ Donation as a Procedure
Another strategy for dealing with this difficulty is one the hand to define end-of-life care as a process and an ethical priority and, on the other, to define organ donation as a strict procedure (quote 7).
Making Sense of the Ethical Dilemma
Participants perceived the gap between theory and practice as “impossible,” “hypocritical,” and “schizophrenic.” The ethical tension appeared to be partly resolved by considering organ donation as a way to give meaning to the patient’s death (quote 8). This consideration is not restricted to the patients themselves but is in fact extended to the future transplant recipients. This utilitarian approach allows healthcare professionals to consider cDCD in a broader benefit-risk balance (quote 9).
Ethical Tensions During the Period Between the Decision to Withdraw Life-Sustaining Treatments and Its Actual Implementation
The tension between end-of-life care and organ donation is particularly evident during this period. Combining taking care of the patient during end of life and organizing the organ donation procedure, with its technical and operational requirements, can be challenging for healthcare professionals.
Experience of Dual Objectives: An Example From the Field Observation
A particular situation led to intense debates within the ICU team. A 36-year-old patient was identified as a potential cDCD donor. During the 48 h required to organize the cDCD procedure, he developed a heparin-induced thrombocytopenia with pulmonary embolism. The question for the team was how to deal with a potential worsening of the situation. Some members of the ICU team felt uncomfortable with this double objective: on the one hand providing end-of-life care and avoiding unnecessary treatments and, on the other hand, preserving the organs before they were retrieved. Each new complication that occurred during this period was an opportunity to discuss the tensions they experienced.
A Difficult Compromise Between End-of-Life Care and Organ Preservation
For half of the interviewed ICU staff members, the introduction or the increase of treatments that are no longer necessary for the patient but that are useful to preserve organ viability raises ethical questions and discomfort (Table 3, quotes 1 and 2). For the other half, and as in the situation described above, a compromise is possible and severe complications should be treated on two conditions: first they should not compromise the organ procurement proposal, and second the patient should be kept under deep and continuous sedation until death (quote 3).
A Time to Support Relatives
The participating nurses were adamant to use this time period to reword the physicians’ explanations and to provide emotional support to the relatives (quote 4). They insisted that special attention was given to the dying patient, which enables the organization of end-of-life rituals (quote 5). Last, this time period also allowed healthcare professionals and relatives to provide active verbal and non-verbal support to the patient, thus encouraging patient-centered care (quote 6).
Ethical Tensions During Dying, Death, and Organ Procurement Procedure
French regulation specifies that, following WLST, the agonic phase—that is, the time running from treatment withdrawal to death—has to be less than 180 min in order to allow organ procurement.
The pressure for Organ Donation Success and Its Potential Impact on End-of-Life Practices
Participants reported increased stress during the implementation of decisions to withdraw LST (Table 4, quote 1), related to the fact that circulatory death must occur within the timeframe required for organ donation to be successful (quotes 2 and 3). This pressure on success can lead to changes in end-of-life practices, particularly regarding sedative practices (quote 4). This potential impact of the cDCD procedure on sedative practices is experienced as difficult for many healthcare professionals (quote 5).
Procedural Failures as a Positive Ethical Signal
A strategy for dealing with this pressure is to define a successful organ donation procedure as one that results in effective organ procurement (quote 6). However, another strategy exists to feel ethically comfortable: many physicians reported that they were reassured when a cDCD procedure failed because the patient didn’t die within the allowed timeframe. This procedural “failure” gives an opportunity to place the patient—rather than the organ donation—at the heart of their practice (quote7).
A Modified Experience of Dying and Death
The systematic use of normothermic regional perfusion offers logistic advantages to the relatives, especially the continuation of end-of-life care in the ICU. However, our field observations showed that end-of-life support was not always optimal and that he atmosphere in the room was deemed as being not appropriate for providing support (quote 8). This difficulty is even more acute when WLST occurs in the operating room where relatives are unable to support the patient and to say goodbye (quote 9). Several participants highlighted the fact that organ procurement is an exceptionally technical procedure (quote 10). Healthcare professionals sometimes take the opportunity to attend the procedure although they are not directly involved in the patient’s care, which was perceived as a form of voyeurism that may further desacralize the patient’s end of life (quote 11). Last, healthcare professionals often felt that they were unable to care for the dying patient as they would have liked to (quote 12). Hence, they felt that they were “stealing the patient’s death” from both the patient him/herself and from the relatives. This was problematic for healthcare professionals who described quality of dying as a major criterion for the quality of their work (quote 13).
Discussion
National policies and guidelines have attempted to shape the process of cDCD into a routine activity for healthcare professionals so that it can become an accepted practice (15, 27). Ethical frameworks imply that healthcare professionals should not experience a moral tension between caring for the dying patient and altering his/her care for the purpose of donation. The interviews conducted during our study show that in practice the situation is more complex for both ICU physicians and nurses with a delicate balance between, on the one hand, end-of-life care and, on the other, organ donation (Figure 1). Indeed there is a gap between ethical theories and practice (28, 29) that clinicians seek to fill the best they can at all stages of the process.
FIGURE 1
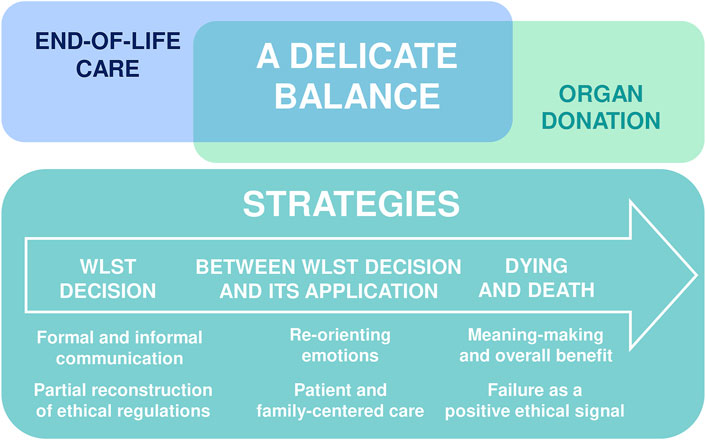
FIGURE 1. Experienced and perceived solutions and strategies.
Concerned simultaneously about end-of-life care and organ donation, healthcare professionals do not want to act against their moral principles and thus develop five types of strategies to solve the ethical and emotional tensions they experience (Figure 1). The first strategy used relies on virtue-centered communication (29). Physicians learn to be demonstrative by staging a distinct temporality between the WLST decision and the organ donation discussion in order to internalize the ethical principal at the basis of cDCD: the separation between WLST decision-making and organ donation decision-making. The second strategy is partial reconstruction of ethical regulations: once the demonstration described above has operated, clinicians can more openly express the intellectual and emotional limits of this practice. The third strategy concerns re-orientating emotions: at the time of WLST decision, some healthcare professionals focus on the WLST decision-making process by relegating organ donation to a secondary organizational and logistical issue. Once the decision to WLST has been made, healthcare professionals may experience important discomforts concerning end-of-life care vs. organ preservation strategies, or tensions concerning the direct exposure of relatives to the organizational dimensions of death. Instead of dwelling on the ethical tensions surrounding the patients’ treatment in anticipation of organ donation, they seek to use the extra time to provide quality support and care to the relatives and to ensure that healthcare professionals and relatives accept and adhere to both the WLST decision and the organ donation project. For some physicians and nurses, this delay may contribute to the quality of the patient’s death by allowing time for the relatives to be at the patient’s side and to say goodbye. The fourth strategy implies defending the principal of “overall benefit”. Indeed when confronted with death in the context of cDCD clinicians can experience moral distress and the feeling of “robbing” the patient’s death. To overcome this tension, the overall benefit of organ donation serves to maintain motivation. The fifth and last strategy implies necessary failures of the cDCD end-of-life procedure: ensuring that failure can happen (i.e., the patient doesn’t die within the timeframe) is a comfort for clinicians in that the quality of the person’s end-of-life takes precedence over the technical procedure.
One important finding of our study is that cDCD procedures are the result of several days of emotional and ethical tension between healthcare professionals, most often shared with the patient’s relatives. cDCD reshapes end of life in ICU, as end-of-life care is not only followed by death but also by organ donation. Despite the above-mentioned strategies, none of the stages of the process are black or white and there are no undisputable solutions to the complexity of the moral tensions experienced. Clinicians navigate in “grey areas,” juggling with official guidelines and ethical dilemmas, as well as with concrete moral, intellectual and emotional difficulties. Their task is to give meaning to the process, a meaning that can be shared with the patients’ family members and among the team (30). These concerns around “ethics in practice” take place within an ICU and, each time, within a specific ethical climate (31).
Healthcare professionals are vital for the implementation of cDCD and their attitudes can influence their participation. Satisfaction with end-of-life care impacts on physicians’ and nurses’ well-being (32) as well as on relatives’ well-being both during and after the patient’s death (33–35). Quality of communication between team members (36), adapted leadership and involvement of nurses (37) at all stages of the process are important elements that will help clinicians overcome these ethical tensions as a group—left alone to deal with these tensions, clinicians could develop moral distress and burnout leading to leaving the ICU (38).
Our study has some limitations. First, it was conducted in a single country (France), with specific end-of-life legislation (13) and cDCD protocols (15). Moreover, it was conducted in a single ICU, one of the first to have implemented this procedure, with a potential impact of the unit culture on the results. However, results of this exploratory single-centre study provide insights into healthcare professionals’ experience that may help design future multicentre studies (39). Last, although our purposive sampling strategy was designed to maximize the diversity of ICU clinicians who participated in the study, our results are—by definition—not entirely generalizable to all healthcare professionals working in ICU. Participation in qualitative interviews was voluntary, creating a possible selection bias: clinicians with difficulties in (or reluctance to) expressing themselves or their experiences concerning the cDCD process may have been omitted. Last, only one researcher coded the interviews. However, to reduce the risk of bias, two other researchers independently coded 3 transcripts for intercoder reliability that proved to be good. Any difficulties or uncertainties encountered by the main coder were discussed and resolved during team meetings.
This qualitative study provides in-depth understanding of the experience of ICU clinicians of the cDCD process. Despite clear and transparent national guidelines, the process remains entangled in a variety of ethical and emotional ambiguities that they strive to solve using various strategies. Overall, ICU clinicians believe that the implementation of cDCD is ethically reasonable as long as end-of-life care is preserved. Taken together, our results indicate that although national guidelines for cDCD are warranted to create a common legal, clinical and ethical framework, the implementation of cDCD in routine practice requires a shared understanding of the difficult compromises experienced by ICU clinicians between end-of life care and organ donation among ICU clinicians.
Data Availability Statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics Statement
All participants provided informed consent, and interview data were anonymized during transcription. The appropriate institutional review board (Comité d’Ethique pour la Recherche en Anesthésie-Réanimation, CERAR No. 2020-127) approved this study.
Author Contributions
ML and NK-B contributed to the conception of the study protocol, the analysis of the data, the draft of the manuscript, approved the manuscript prepared for publication, and agreed to be accountable for all aspects of the work. SM contributed to the conception of the study protocol, the acquisition and the analysis of the data, approved the manuscript prepared for publication, and agreed to be accountable for all aspects of the work. EC-I contributed to the analysis of data, approved the manuscript prepared for publication, and agreed to be accountable for all aspects of the work. FR contributed to the conception of the study protocol, approved the manuscript prepared for publication, and agreed to be accountable for all aspects of the work. AM critically revised the work for important intellectual content, approved the manuscript prepared for publication, and agreed to be accountable for all aspects of the work. LM critically revised the work for important intellectual content, approved the manuscript prepared for publication, and agreed to be accountable for all aspects of the work.
Funding
A source of funding was provided by the Fondation de France and was used for the transcription of the interviews. The funding source had no role in the design and conduct of the study.
Conflict of Interest
ML and FR are members of the steering committee of the French cDCD program.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontierspartnerships.org/articles/10.3389/ti.2022.10648/full#supplementary-material
References
1. Thuong, M, Ruiz, A, Evrard, P, Kuiper, M, Boffa, C, Akhtar, MZ, et al. New Classification of Donation after Circulatory Death Donors Definitions and Terminology. Transpl Int (2016) 29(7):749–59. doi:10.1111/tri.12776
2. Savier, E, Lim, C, Rayar, M, Orlando, F, Boudjema, K, Mohkam, K, et al. Favorable Outcomes of Liver Transplantation from Controlled Circulatory Death Donors Using Normothermic Regional Perfusion Compared to Brain Death Donors. Transplantation (2020) 104(9):1943–51. doi:10.1097/TP.0000000000003372
3. Antoine, C, Jasseron, C, Dondero, F, and Savier, E. Liver Transplantation from Controlled Donors after Circulatory Death Using Normothermic Regional Perfusion: An Initial French Experience. Liver Transpl (2020) 26(11):1516–21. doi:10.1002/lt.25818
4. Savoye, E, Legeai, C, Branchereau, J, Gay, S, Riou, B, Gaudez, F, et al. Optimal Donation of Kidney Transplants after Controlled Circulatory Death. Am J Transpl (2021) 18:2424–36. doi:10.1111/ajt.16425
5. Weiss, J, Elmer, A, Mahíllo, B, Dominguez-Gil, B, Avsec, D, Nanni Costa, A, et al. Evolution of Deceased Organ Donation Activity versus Efficiency over a 15-year Period: An International Comparison. Transplantation (2018) 102(10):1768–78. doi:10.1097/TP.0000000000002226
6. Smith, M, Dominguez-Gil, B, Greer, DM, Manara, AR, and Souter, MJ. Organ Donation after Circulatory Death: Current Status and Future Potential. Intensive Care Med (2019) 45(3):310–21. doi:10.1007/s00134-019-05533-0
7. Lomero, M, Gardiner, D, Coll, E, Haase-Kromwijk, B, Procaccio, F, Immer, F, et al. .Donation after Circulatory Death Today: an Updated Overview of the European Landscape. Transpl Int (2020) 33(1):76–88. doi:10.1111/tri.13506
8. Myburgh, J, Abillama, F, Chiumello, D, Dobb, G, Jacobe, S, Kleinpell, R, et al. End-of-life Care in the Intensive Care Unit: Report from the Task Force of World Federation of Societies of Intensive and Critical Care Medicine. J Crit Care (2016) 34:125–30. doi:10.1016/j.jcrc.2016.04.017
9. Lesieur, O, Herbland, A, Cabasson, S, Hoppe, MA, Guillaume, F, and Leloup, M. Changes in Limitations of Life-Sustaining Treatments over Time in a French Intensive Care Unit: A Prospective Observational Study. J Crit Care (2018) 47:21–9. doi:10.1016/j.jcrc.2018.05.018
10. Sprung, CL, Ricou, B, Hartog, CS, Maia, P, Mentzelopoulos, SD, Weiss, M, et al. .Changes in End-Of-Life Practices in European Intensive Care Units from 1999 to 2016. JAMA 322:1692–704. doi:10.1001/jama.2019.14608
11. Puybasset, L, Bazin, JE, Beloucif, S, Bizouarn, P, Crozier, S, Devalois, B, et al. Critical Appraisal of Organ Procurement under Maastricht 3 Condition. Ann Fr Anesth Reanim (2014) 33(2):120–7. doi:10.1016/j.annfar.2013.11.004
12. Graftieaux, JP, Bollaert, PE, Haddad, L, Kentish-Barnes, N, Nitenber, G, Robert, R, et al. Contribution of the Ethics Committee of the French Society of Intensive Care Medicine to a Scenario for the Implementation of Organ Donation after Maastricht III-type Cardiac Death in France. Ann Fr Anesth Reanim (2014) 33(2):128–34. doi:10.1016/j.annfar.2014.01.003
13. Le Dorze, M, Kandelman, S, and Veber, B, SFAR’s Ethics Committee. End-of-life Care in the French ICU: Impact of Claeys-Leonetti Law on Decision to Withhold or Withdraw Life-Supportive Therapy. Anaesth Crit Care Pain Med (2019) 38(6):569–70. doi:10.1016/j.accpm.2019.10.013
14. Le Dorze, M, Kandelman, S, and Veber, B, SFAR Ethics Committee. Deep Continuous Sedation Maintained until Death, in French Intensive Care Units. Anaesth Crit Care Pain Med (2019) 39:115–6. doi:10.1016/j.accpm.2019.07.008
15. Corinne, A, Bronchard, R, and Durin, L. Direction générale médicale et scientifique de l’Agence de la Biomédecine, Paris, France. Conditions for Recovery of Organs after Circulatory Arrest (Maastricht Category 3) in a Health Care Facility Authorized to Recover Organs (2019). Available from: https://www.agence-biomedecine.fr/IMG/pdf/v7_guide_ddac_miii_novembre_2019_eng.pdf (Accessed March 5, 2022).
16. Mandell, MS, Zamudio, S, Seem, D, McGaw, LJ, Wood, G, Liehr, P, et al. National Evaluation of Healthcare Provider Attitudes toward Organ Donation after Cardiac Death. Crit Care Med (2006) 34(12):2952–8. doi:10.1097/01.CCM.0000247718.27324.65
17. D’Alessandro, AM, Peltier, JW, and Phelps, JE. Understanding the Antecedents of the Acceptance of Donation after Cardiac Death by Healthcare Professionals. Crit Care Med (2008) 36(4):1075–81. doi:10.1097/CCM.0b013e3181691b2b
18. Bastami, S, Matthes, O, Krones, T, and Biller-Andorno, N. Systematic Review of Attitudes toward Donation after Cardiac Death Among Healthcare Providers and the General Public. Crit Care Med (2013) 41(3):897–905. doi:10.1097/CCM.0b013e31827585fe
19. Kentish-Barnes, N, Duranteau, J, Montlahuc, C, Charpentier, J, Martin-Lefevre, L, Joseph, L, et al. Clinicians’ Perception and Experience of Organ Donation from Brain-Dead Patients. Crit Care Med (2017) 45(9):1489–99. doi:10.1097/CCM.0000000000002581
20. Hart, JL, Kohn, R, and Halpern, SD. Perceptions of Organ Donation after Circulatory Determination of Death Among Critical Care Physicians and Nurses: a National Survey. Crit Care Med (2012) 40(9):2595–600. doi:10.1097/CCM.0b013e3182590098
21. Lee, YY, Ranse, K, Silvester, W, Mehta, A, and Van Haren, F. Attitudes and Self-Reported End-Of-Life Care of Australian and New Zealand Intensive Care Doctors in the Context of Organ Donation after Circulatory Death. Anaesth Intensive Care (2018) 46(5):488–97. doi:10.1177/0310057X1804600510
22. Jones, J, and Smith, J. Ethnography: Challenges and Opportunities. Evid Based Nurs (2017) 20(4):98–100. doi:10.1136/eb-2017-102786
23. Malterud, K. Qualitative Research: Standards, Challenges, and Guidelines. Lancet (2001) 358(9280):483–8. doi:10.1016/S0140-6736(01)05627-6
24. Saunders, B, Sim, J, Kingstone, T, Baker, S, Waterfield, J, Bartlam, B, et al. Saturation in Qualitative Research: Exploring its Conceptualization and Operationalization. Qual Quant (2018) 52(4):1893–907. doi:10.1007/s11135-017-0574-8
25. Braun, V, and Clarke, V. Using Thematic Analysis in Psychology. Qual Res Psychol (2006) 3(2):77–101. doi:10.1191/1478088706qp063oa
26. DeCuir-Gunby, J, Marshall, P, and Mcculloch, A. Developing and Using a Codebook for the Analysis of Interview Data: An Example from a Professional Development Research Project. Field Methods (2011) 23:136–55. doi:10.1177/1525822X10388468
27. Cooper, J. Problematising the Ethics of Organ Donation after Circulatory Death in the UK. Crit Public Health (2017) 27(4):499–505. doi:10.1080/09581596.2016.1225948
28. Madani, M, Larijani, B, Madani, E, and Ghasemzadeh, N. Establishment of Medical Education upon Internalization of Virtue Ethics: Bridging the gap between Theory and Practice. J Med Ethics Hist Med (2017) 10:3.
29. Madani, M, Vedadhir, A, Larijani, B, Khazaei, Z, and Gharamaleki, AF. Bridging the Gap between Ethical Theory and Practice in Medicine: A Constructivist Grounded Theory Study. Sci Eng Ethics (2020) 26(4):2255–75. doi:10.1007/s11948-020-00217-1
30. Kentish-Barnes, N, Davidson, JE, and Cox, CE. Family Presence during Cardiopulmonary Resuscitation: an Opportunity for Meaning-Making in Bereavement. Intensive Care Med (2014) 40(12):1954–6. doi:10.1007/s00134-014-3396-3
31. Van den Bulcke, B, Metaxa, V, Reyners, AK, Rusinova, K, Jensen, HI, Malmgren, J, et al. Ethical Climate and Intention to Leave Among Critical Care Clinicians: an Observational Study in 68 Intensive Care Units across Europe and the United States. Intensive Care Med (2020) 46(1):46–56. doi:10.1007/s00134-019-05829-1
32. Boissier, F, Seegers, V, Seguin, A, Legriel, S, Cariou, A, Jaber, S, et al. Assessing Physicians’ and Nurses’ Experience of Dying and Death in the ICU: Development of the CAESAR-P and the CAESAR-N Instruments. Crit Care (2020) 24(1):521. doi:10.1186/s13054-020-03191-z
33. Kentish-Barnes, N, Chaize, M, Seegers, V, Legriel, S, Cariou, A, Jaber, S, et al. Complicated Grief after Death of a Relative in the Intensive Care Unit. Eur Respir J (2015) 45(5):1341–52. doi:10.1183/09031936.00160014
34. Kentish-Barnes, N, and Azoulay, E. The Challenge of Addressing Family Needs at the End of Life. Am J Respir Crit Care Med (2016) 193(2):108–10. doi:10.1164/rccm.201509-1913ED
35. Kentish-Barnes, N, Seegers, V, Legriel, S, Cariou, A, Jaber, S, Lefrant, JY, et al. CAESAR: a New Tool to Assess Relatives’ Experience of Dying and Death in the ICU. Intensive Care Med (2016) 42(6):995–1002. doi:10.1007/s00134-016-4260-4
36. Azoulay, E, Forel, JM, Vinatier, I, Truillet, R, Renault, A, Valade, S, et al. Questions to Improve Family-Staff Communication in the ICU: a Randomized Controlled Trial. Intensive Care Med (2018) 44(11):1879–87. doi:10.1007/s00134-018-5423-2
37. Kentish-Barnes, N, Chevret, S, and Azoulay, E. Guiding Intensive Care Physicians’ Communication and Behavior towards Bereaved Relatives: Study Protocol for a Cluster Randomized Controlled Trial (COSMIC-EOL). Trials (2018) 19(1):698. doi:10.1186/s13063-018-3084-7
38. Vincent, H, Jones, DJ, and Engebretson, J. Moral Distress Perspectives Among Interprofessional Intensive Care Unit Team Members. Nurs Ethics (2020) 27(6):1450–60. doi:10.1177/0969733020916747
39.Assistance Publique - Hôpitaux de Paris. Experience Of Relatives And Caregivers Of Death In ICU After The Withdrawal Of Life-Sustaining Therapies, Associated With An Organ Procurement Procedure (Controlled Donation after Circulatory Death). clinicaltrials.Gov (2021). Available at: https://clinicaltrials.gov/ct2/show/NCT05041023 (Accessed March 5, 2022).
Keywords: organ donation, qualitative research, end of life, controlled donation after circulatory death, withdrawal of life-sustaining treatments
Citation: Le Dorze M, Martouzet S, Cassiani-Ingoni E, Roussin F, Mebazaa A, Morin L and Kentish-Barnes N (2022) “A Delicate balance”—Perceptions and Experiences of ICU Physicians and Nurses Regarding Controlled Donation After Circulatory Death. A Qualitative Study. Transpl Int 35:10648. doi: 10.3389/ti.2022.10648
Received: 16 May 2022; Accepted: 23 August 2022;
Published: 06 September 2022.
Copyright © 2022 Le Dorze, Martouzet, Cassiani-Ingoni, Roussin, Mebazaa, Morin and Kentish-Barnes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matthieu Le Dorze, matthieu.ledorze@aphp.fr