 Dennis A. J. van den Broek1*†
Dennis A. J. van den Broek1*† Soufian Meziyerh1†
Soufian Meziyerh1† Klemens Budde2†
Klemens Budde2† Carmen Lefaucheur3†
Carmen Lefaucheur3† Emanuele Cozzi4†
Emanuele Cozzi4† Dominique Bertrand5Covadonga López del Moral2,6†
Dominique Bertrand5Covadonga López del Moral2,6† Anthony Dorling7†Marie-Paule Emonds8,9†
Anthony Dorling7†Marie-Paule Emonds8,9† Maarten Naesens9†
Maarten Naesens9† Aiko P. J. de Vries1† and the ESOT Working Group Subclinical DSA Monitoring on behalf of the ESOT Guidelines Taskforce
Aiko P. J. de Vries1† and the ESOT Working Group Subclinical DSA Monitoring on behalf of the ESOT Guidelines Taskforce- 1Division of Nephrology, Department of Medicine, Leiden Transplant Center, Leiden University Medical Center, Leiden University, Leiden, Netherlands
- 2Department of Nephrology and Medical Intensive Care, Charité Universitätsmedizin Berlin, Berlin, Germany
- 3Paris Translational Research Center for Organ Transplantation, Kidney Transplant Department, Saint Louis Hospital, Université de Paris Cité, Paris, France
- 4Department of Cardiac, Thoracic and Vascular Sciences and Public Health, Transplant Immunology Unit, Padua University Hospital, Padua, Italy
- 5Department of Nephrology, Transplantation and Hemodialysis, Rouen University Hospital, Rouen, France
- 6Valdecilla Biomedical Research Institute (IDIVAL), Santander, Spain
- 7Department of Inflammation Biology, Centre for Nephrology, Urology and Transplantation, School of Immunology & Microbial Sciences, King’s College London, Guy’s Hospital, London, United Kingdom
- 8Histocompatibility and Immunogenetics Laboratory (HILA), Belgian Red Cross-Flanders, Mechelen, Belgium
- 9Department of Microbiology, Immunology and Transplantation, KU Leuven, Leuven, Belgium
Solid phase immunoassays improved the detection and determination of the antigen-specificity of donor-specific antibodies (DSA) to human leukocyte antigens (HLA). The widespread use of SPI in kidney transplantation also introduced new clinical dilemmas, such as whether patients should be monitored for DSA pre- or post-transplantation. Pretransplant screening through SPI has become standard practice and DSA are readily determined in case of suspected rejection. However, DSA monitoring in recipients with stable graft function has not been universally established as standard of care. This may be related to uncertainty regarding the clinical utility of DSA monitoring as a screening tool. This consensus report aims to appraise the clinical utility of DSA monitoring in recipients without overt signs of graft dysfunction, using the Wilson & Junger criteria for assessing the validity of a screening practice. To assess the evidence on DSA monitoring, the European Society for Organ Transplantation (ESOT) convened a dedicated workgroup, comprised of experts in transplantation nephrology and immunology, to review relevant literature. Guidelines and statements were developed during a consensus conference by Delphi methodology that took place in person in November 2022 in Prague. The findings and recommendations of the workgroup on subclinical DSA monitoring are presented in this article.
Introduction
The introduction of the complement-dependent cytotoxicity assay (CDC) in 1969 was the first step towards addressing the deleterious consequences of the humoral immune response and antibody-mediated rejection (ABMR) [1]. Means to investigate these entities were further expanded in later years by the introduction of novel techniques, amongst others, flow-cytometry and solid phase immunoassays (SPI). The use of the sensitive SPI also introduced new dilemmas, such as how to interpret SPI results in case of a negative pretransplant CDC-crossmatch or whether patients should be monitored for the incidence of donor-specific antibodies (DSA) to human leukocyte antigens (HLA) post-transplantation. A consensus meeting in 2013 concluded that pretransplant screening for potential DSA via single-antigen bead (SAB) SPI could be of benefit in risk stratification [2]. As a result, organ allocation organizations have mandated pretransplant screening of HLA antibodies through SAB-SPI as immunological risk stratification in order to define non-acceptable HLA antigens [3]. A recent position paper on pretransplant immunologic risk stratification adds further arguments for this screening practice [4]. Post-transplant monitoring of DSA in patients with graft dysfunction seems to be equally standard practice in case of clinical suspicion of ABMR [5, 6]. However, standardized monitoring of DSA in kidney transplant recipients (KTR) without signs of overt transplant dysfunction, so called subclinical DSA, has not universally taken hold as standard of care in most transplant centers. This is likely related to uncertainty regarding the clinical utility of standardized monitoring for subclinical DSA. The main aim of subclinical DSA monitoring is to identify patients who are at greater risk for rejection, either incipient or future, which makes it a form of (transplant) population screening. For such a strategy to have clinical utility, diagnostic and therapeutic ramifications need to be defined in case a patient is identified through screening and these consequences should lead to improved graft and patient outcomes. This may relate to earlier diagnosis and treatment of underlying subclinical rejection, but perhaps also to adaptation of maintenance treatment strategies to prevent future rejection. Additionally, cost-effectiveness of such practices should be considered. While DSA monitoring in stable patients has been recommended in previous guidelines, potential benefits of its consequences were largely unknown, especially in regards to treatment of underlying subclinical rejection [2]. This could possibly explain why some centers were hesitant to implement such strategies. However, uncertainties regarding effective therapeutic ramifications may counteract potential benefits of early detection. This limits potential further improvements in long-term allograft survival from an ontological reductionist view on alloimmunity. In the wake of new developments in this field over the past decade, this consensus report aims to appraise the clinical utility of regular standardized post-transplant monitoring of DSA in stable KTR. We will utilize the criteria for successful screening as developed by Wilson & Jungner in 1964, to ensure that all relevant aspects are reviewed [7] (Table 1). Additionally, potential knowledge gaps are identified and future research objectives stated.
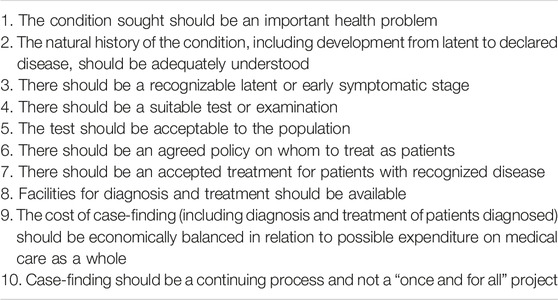
TABLE 1. Wilson & Jungner’s principles of screening.
To formulate this consensus statement, the European Society for Organ Transplantation (ESOT) convened a consensus conference, comprised of a European panel of experts in transplantation nephrology and immunology. The aim of this conference was to develop guidelines on DSA monitoring. The panel and juries were presented with summaries of evidence. Consensus statements and recommendations, and the Wilson & Jungner criteria they reflect, are summarized in Table 2. This document, which will be updated to reflect new evidence as it becomes available, is intended for healthcare providers.
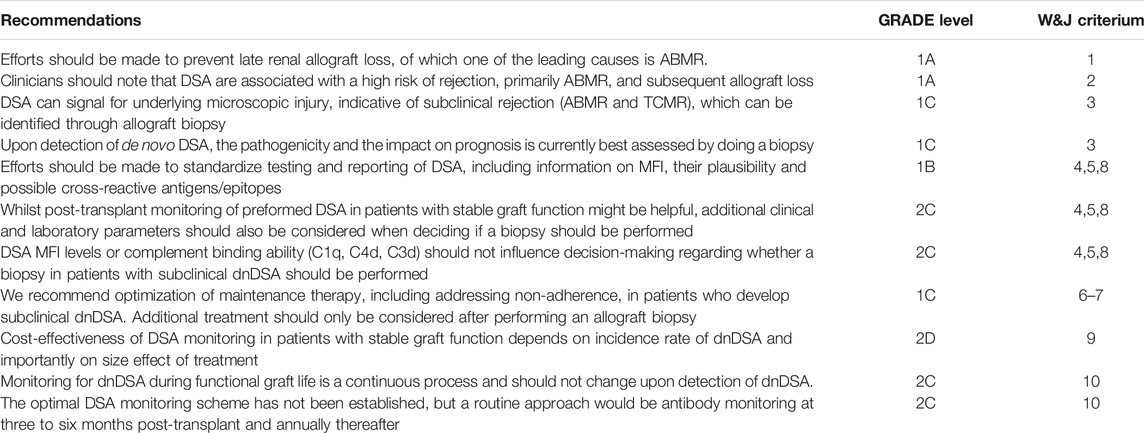
TABLE 2. Summary of statements and recommendations.
Methods
The consensus development process was organized by a dedicated Guidelines Taskforce within ESOT and its sections ELITA, EKITA, EPITA, ECTTA, ETHAP, Education Committee, YPT, Transplant International editorial board members and patient representatives. The detailed description of methodology used is reported previously [8]. Briefly, key issues were identified by each workgroup and specific clinical questions were formulated according to the PICO methodology (PICO = Population, Intervention, Comparator and Outcome). All PICO questions are listed in Table 3. Following the definition of the PICOs, literature searches were developed by expert staff from the Centre for Evidence in Transplantation, who have expertise in conducting systematic reviews and subsequently integrated, when needed, by the steering committee experts. The workgroup proposed a recommendation for each key question, based on the quality of evidence rated using the GRADE approach, with high quality rated as A, medium quality as B, and low quality as C; very low quality of evidence was not considered. For evaluation of the quality of evidence according to GRADE the following features were considered: study design, risk of bias, inconsistency, indirectness, imprecision, number of patients, effect, importance and publication bias. Strength of recommendation was rated as 1 (strong) or 2 (weak).
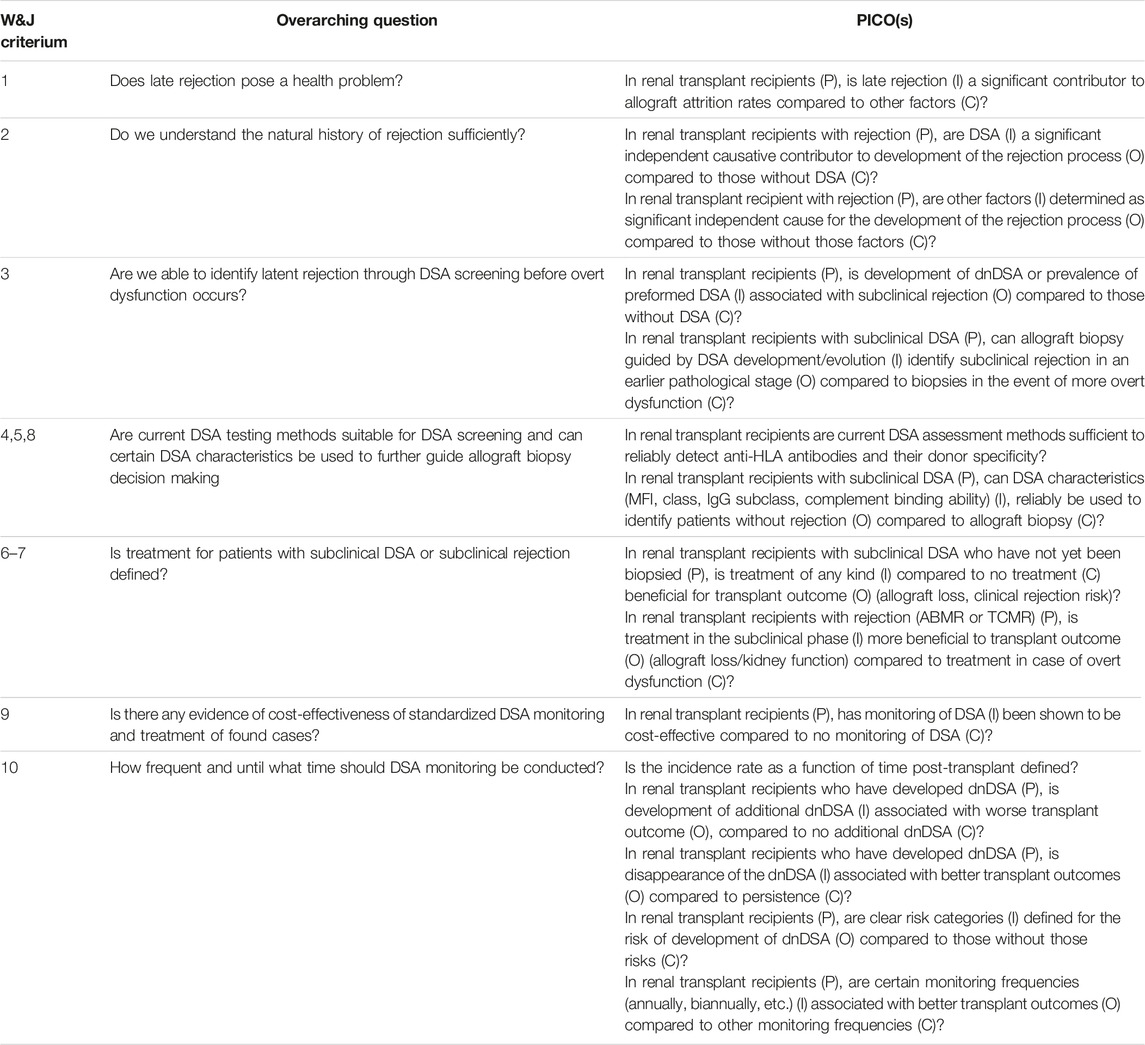
TABLE 3. Overarching questions & PICOs.
The Delphi method was applied to arrive at a group opinion during the consensus conference. Complete information, including the list of consensus conference workgroup domains and topics, and the process regarding consensus conference participant selection, development and refinement of consensus statements, and modified Delphi methodology including consensus polling, were determined before the conference held in Prague, Czech Republic, November 13–15, 2022, as previously reported [8] Table 3.
Efforts Should Be Made to Prevent Late Renal Allograft Loss, of Which One of the Leading Causes Is ABMR. (1A)
For a successful screening strategy it is important that the disease is relevant and constitutes an significant health problem. Breakthroughs in maintenance immunosuppression during the latter part of the past century drastically increased kidney graft survival rates [9]. This was, however, realized mainly through increases in graft survival over the first year. Comparably less progress has been made in improving graft attrition rates beyond the first year during this era. However, more recent European analysis of collaborative transplant study (CTS) data showed that improvement of long-term graft survival since 2000 was greater than short-term advancement, independently of changing donor and recipient characteristics, likely reflecting the evolutions in posttransplant monitoring and management [10, 11]. An important limiting factor to prolong long-term death-censored graft survival is the development of antibody-mediated rejection (ABMR), in which DSA play an important role [12]. This entity is recognized as a major cause for overall death-censored renal allograft loss in recent decades [13, 14]. The Banff ’19 pathology classification recognizes three forms of ABMR in renal allografts: active, chronic active and chronic ABMR [5]. Even though there is incidental empiric evidence for reversal in the case of (hyper)active forms of ABMR [15], all forms of ABMR infer a great risk for graft failure [16]. A recent analysis attributed around a third of all allograft loss to ABMR, particularly contributing to late allograft failure [17]. Therefore, it seems undisputable that diminishing the rate of allograft loss due to ABMR is an important health issue in kidney transplantation and we recommend that efforts to further improve long-term graft survival should explore new openings to steer away from the current diagnostic and therapeutic nihilistic view on chronic rejection.
Clinicians Should Note That DSA Are Associated With a High Risk of Rejection, Primarily ABMR, and Subsequent Allograft Loss. (1A)
Epidemiological Associations Between HLA-DSA and Allograft Outcome
For screening to be successful, one should have an understanding of how underlying pathological processes can develop into overt graft dysfunction.
In case of ABMR, the screening marker itself seems to be implicated in the underlying pathological process [6, 12]. This is apparent with pretransplant DSA, considering the high risk of hyperacute rejection if transplantation proceeds despite a positive CDC-crossmatch. Modern practice precludes such transplantation with pretransplant listing of non-acceptable HLA antigens, or with measures such as paired kidney exchange programs or desensitization in the living donation setting. In contrast, CDC-crossmatch negative pretransplant DSA, which are identified through SPI only, are not necessarily a contraindication to transplantation in patients faced with no alternatives beyond dialysis [3]. However, these DSA still convey increased risk for ABMR and allograft loss according to a meta-analysis by Mohan et al. [18] Recent analysis of CTS data indicated that nearly 15% of recipients of deceased donor kidneys with crossmatch negative pretransplant DSA progressed to allograft failure within the first year post-transplant [19]. This figure was even higher in retransplant patients. In regards to dnDSA, a large meta-analysis by Sharma et al. [20] implicated development of dnDSA as a severe risk factor for notably cellular rejection, acute ABMR (aABMR), chronic ABMR (cABMR), and allograft loss. Moreover, CTS data showed that 20% of patients who developed dnDSA in the first post-transplant year progressed to allograft failure within the next five [19]. A recent randomized trial corroborated these results [21].
Pathogenesis of HLA-DSA and Plausible Causality With Subsequent Rejection
The genesis of DSA after transplantation is a complex process. B-cells can initiate and subsequently differentiated plasma cells (as well as B-cells) can maintain production of these antibodies as a result of sensitization of the adaptive immune system. Sensitization could be related to a period of underexposure, either due to non-adherence or iatrogenic reduction of immunosuppression [22–28]. Additionally, poor HLA matching [28–31] and previous episodes of T-cell mediated rejection (TCMR) [29, 30, 32–34] have been associated with DSA development. Other risk factors pertain to certain recipient characteristics such as age or ethnicity [35, 36]. The association of previous TCMR and dnDSA development is hypothesized to be explained by sensitization of the B-cell compartment through inflammation induced by T-cell alloimmunity, especially T-follicular helper cells [37–39]. The role of T-cells in a process which could ultimately lead to ABMR seems to question the dichotomous view on rejection (i.e., either TCMR or ABMR as separate entities). Perhaps a more contemporary view on rejection is that it is a heterogenous spectrum with different histological and clinical manifestations [40].
While the process of sensitization leading to DSA formation is complex and multifactorial, the risks DSA convey are clear. Still, this does not necessarily infer a causal relationship. Though the pathogenicity of HLA-DSA was extensively studied in recent years and a recent thorough literature review by Callemeyn et al. [40] attempted to untangle association from causation. This review assessed the possible causal relationship between HLA-DSA and microvascular inflammation (MVI), a histopathological hallmark of ABMR, through the Bradford-Hill criteria, which can be used as guide for causal inference in epidemiological research. These criteria include: strength of effect size and reproducibility, experimental evidence in vitro and in vivo, temporality between HLA-DSA appearance and graft injury, biological gradient, and coherence and analogy [40, 41]. Callemeyn et al; [40] illustrates that most criteria are met. However, more investigations are warranted to demonstrate a clear biological gradient between antibody titre and occurrence of ABMR or graft failure; [42]. Yet, recent studies by Viglietti et al; [43, 44] showed that treatment of ABMR through plasmapheresis (PP), intravenous immunoglobulins (IVIG) and rituximab is associated with a significant decrease in DSA MFI and capacity to bind C1q. Interestingly, these reductions in DSA properties were significantly associated with improved graft survival in patients with ABMR. However, treatment effects on more chronic or late ABMR are variable [15]. Furthermore, the histological presentation of ABMR including MVI is not always specific for antibody involvement, as other causes could appear clinicopathologically similar. Nonetheless, there seems to be clear preclinical and clinical evidence of a pathogenic relation between HLA-DSA and ABMR.
Mechanisms of HLA-DSA-Induced Allograft Damage to Explain Phenotypic Variability
Despite this strong relationship, not all recipients with preformed DSA or dnDSA seem to progress to ABMR or graft failure [16, 29, 45]. Multiple mechanisms have been proposed to explain this variation in effect of HLA-DSA on graft outcomes. A recent comprehensive review has summarized HLA-DSA attributes and discussed mechanisms of HLA-DSA-induced effector functions in mediating allograft damage [46]. These effector functions may be Fc-dependent, such as the impact of antibody glycosylation status on complement activation and recruitment of cytotoxic NK-cells and macrophages [47, 48]. Regarding Fc-independent mechanisms, recent studies describe intracellular signalling downstream of HLA-antibody binding to endothelial cells that promote upregulation of adhesion molecules, proliferation and activation of endothelial cells, induction of dendritic cells and CD4+ T-cell maturation [46, 49, 50]. HLA-antibody ligation of the HLA-molecule of endothelial cells can also lead to anaphylatoxin production that can result in more monocyte recruitment. Recruitment is also mediated by the cellular expression of anaphylatoxin receptors on CD4+ and CD8+ T cells, and myeloid cells [51, 52]. Lastly, regulatory T and B-cell populations may play a pivotal role in suppressing the deleterious effects of DSA on the graft. Recent research indicates that these cell lines impart tolerogenic effects through impairment of the T-follicular helper cell – B-cell interaction and that these regulatory cells were significantly reduced in frequency in patients with DSA who developed ABMR, as compared to patients with DSA but absent ABMR [38, 39, 53].
Relationship Between HLA-DSA Properties and Allograft Injury Phenotypes
Several studies have shown that high titre HLA-DSA reflected by high MFI levels, and inflammatory isotype switching toward IgG1 and IgG3, and thus their capacity to bind C1q or C3d are associated with significantly increased microvascular inflammation and C4d deposition [54, 55]. Although considered classically non-inflammatory, the IgG4 isotype has been associated with subclinical graft rejection, including ABMR, in several studies in kidney and other solid organ transplants [55, 56]. Subclinical ABMR was shown to lead to significantly more transplant glomerulopathy and accelerated graft loss when compared to subclinical TCMR [57]. In addition to subclinical ABMR, HLA-DSA have been shown to be significantly associated with kidney graft fibrosis and subsequent accelerated graft loss [58]. The relationship between HLA-DSA and graft fibrosis was independent of previous ABMR episodes. Thus, HLA-DSA, even detected at low strength/MFI, are associated with subclinical damage and fibrosis independent of clinical ABMR occurrence [58, 59].
HLA-DSA Independent Mechanisms of Microvascular Inflammation
Lastly, it must be mentioned that not all patients with MVI, indicative of injury attributed as being “antibody-mediated” by current Banff criteria, have detectable levels of HLA-DSA. The histopathologic entity of MVI without detectable HLA-DSA by definition suggests that factors other than HLA-DSA may mediate MVI, such as non-HLA antibodies [60–63]. Antibody-independent pathways may include NK-cell alloimmunity through a “missing-self” mechanism [64, 65] or direct allorecognition by monocytes [66, 67]. Other causes may not even be related directly to alloimmunity, such as recurrent complement-mediated renal disease, ischemia/reperfusion injury, or viral endothelial infection.
The above presented body of evidence illustrates that there are likely multiple individual pathways, not all of which are fully understood, that eventually lead to varying levels of microscopic injury that is currently defined as MVI and ABMR, which may need some clarification [6, 68]. Nonetheless, regardless of the incompletely understood natural history of ABMR and MVI, there is a large amount of preclinical and clinical evidence warranting strong support for the notion that anti-HLA-DSA are significantly associated with, and predictive of rejection and clinicians should be aware of this [5, 12, 15, 40].
DSA can Be a Signal for Underlying Microscopic Injury, Indicative of Subclinical Rejection (ABMR and TCMR), Which can Be Identified Through Allograft Biopsy. (1C)
Subclinical DSA as a Marker for Latent Rejection
For a valid screening strategy for disease, clinicians should also be able to identify a latent stage. In some cases, patients undergoing rejection present with clinical dysfunction of the graft as first sign. However, most have a latent phase with prevalent DSA prior to developing graft dysfunction. The first evidence of subclinical DSA as a marker for latent rejection came from preclinical studies in a non-human primate model with sequential protocol biopsies by Smith et al. [69, 70] They showed that development of dnDSA generally precedes graft dysfunction, as well as C4d-deposition or transplant glomerulopathy. Clinical studies of longitudinal protocol biopsies in stable renal transplant recipients with preformed DSA show substantial oscillations characterized by fluctuations in HLA-DSAs, C4d deposition and scores for glomerulitis and/or capillaritis in a dynamic and multidirectional fashion [71–73]. Seminal papers by Wiebe et al. [22, 34] have shown that this progressive subclinical injury can also be detected in patients with dnDSA several years after kidney transplantation. They found that of 64 patients who developed dnDSA, the majority was without graft dysfunction. Additionally, development of subclinical dnDSA was independently associated with transplant glomerulopathy (and thus chronic ABMR (cABMR)), decline in graft function, and allograft loss. Therefore, it is unlikely that chronic rejection is the result of a single spike of HLA-DSA or a single episode of ABMR. Instead, it represents a dynamic process that continues, unabated, at varying levels and eventually progresses towards chronic allograft injury, graft dysfunction and ultimately graft loss [12].
Development of latent rejection in patients with subclinical DSA has been observed in other types of organ transplants [74–76], as well as in more recent clinical studies in KTR, which show underlying rejection in roughly half of overall patients (Table 4). Bertrand et al. [77] recently analyzed 123 patients with subclinical dnDSA in a French multicenter cohort study and found that 41.5% of these patients had subclinical ABMR. Loupy et al. [57] showed in a large prospective cohort study of 1,001 patients with 1 year protocol biopsies that of 256 patients with subclinical DSA, 55% had ABMR. Of these cases, 78% were related to pretransplant DSA, further indicating that both pretransplant DSA and dnDSA can underlie a latent pathological process. Coemans et al. [78] recently studied longitudinal protocol and indication biopsies in a single-centre cohort of 1,000 Belgian patients. Of these, 108 had pretransplant DSA and 47 developed dnDSA. The prevalence of subclinical aABMR in protocol biopsies at 3, 12, 24 and 60 months post-transplant was 42.5%, 40.5%, 37.3% and 13.3% respectively in patients with HLA-DSA. Prevalence of transplant glomerulopathy increased over time and this was associated with previously diagnosed aABMR, further corroborating the notion that ABMR is a dynamic and continuous process [71, 72]. Schinstock et al. [30] retrospectively analyzed a single center cohort of patients with serial surveillance biopsies, but also included biopsies at graft dysfunction and upon subclinical dnDSA development. They found that of the 40 patients who were biopsied at the time of dnDSA development, 25%, 7.5% and 20% had underlying aABMR, cABMR, and TCMR respectively. Yamamoto et al. [79] reported on a Japanese cohort of 43 patients with subclinical dnDSA and found that 41.8% of patients had ABMR. Parajuli et al. [80] showed in an American retrospective single center cohort study with biopsies in case of dnDSA development or clinical indication that of 29 patients with subclinical dnDSA, 15 (51%) had underlying rejection. Of those rejections, 60% were ABMR, 20% mixed rejections, and 20% were TCMR. Waldecker et al. [81] retrospectively studied 84 German patients with indication biopsies or in case of dnDSA development from a single centre and found that out of 50 patients with subclinical dnDSA, 44% had ABMR, 15% had TCMR, 12% had mixed rejection and 15% had borderline rejection. Notably, only 14% of these patients had no histopathological signs of rejection at light microscopy. Eskandary et al. [82] retrospectively reported on the screening process for the BORTEJECT study, whereby 861 patients with stable grafts were cross-sectionally screened for presence of DSA [82]. Of 86 patients with subclinical DSA, 44 (51%) met the Banff criteria for ABMR. Lastly, Cornell et al. [83] analysed the results of a prospective trial on pretransplant desensitization with eculizumab in patients with a positive flow-crossmatch and compared the long-term outcomes to a historical matched cohort. The overall prevalence of subclinical ABMR at 3 months, 1 year and 2 years post-transplant was 41.8%, 37% and 20% respectively in a total of 78 patients.
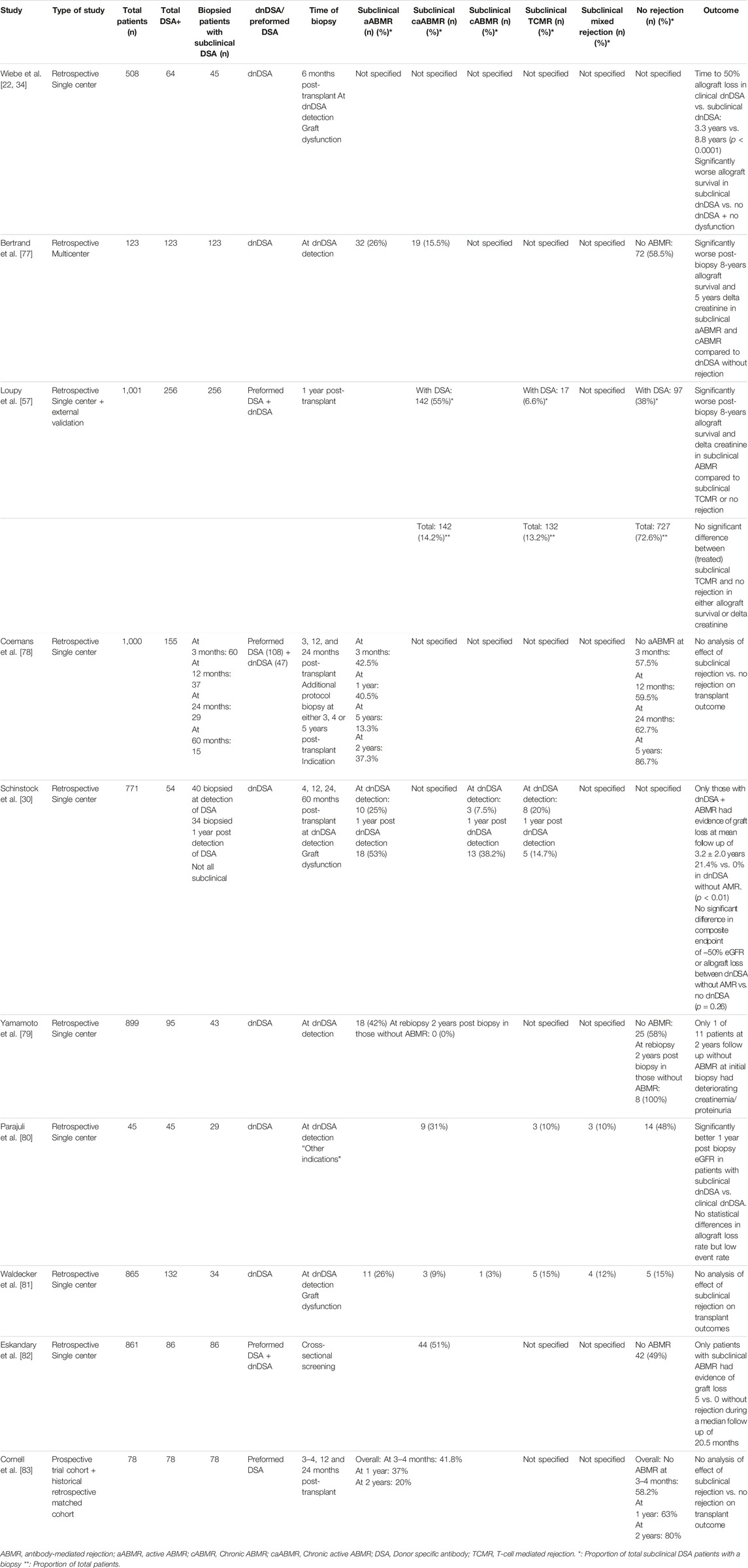
TABLE 4. Summary of studies on subclinical DSA in renal transplant recipients.
Relationship Between de novo DSA and Subclinical T-cell Mediated Rejection
While most studies only reported these biopsy results in terms of either positive or negative for ABMR, the studies by Schinstock et al. [30], Parajuli et al. [80] and Waldecker et al. [81] interestingly further show that subclinical dnDSA can also be a signal for underlying TCMR. Unfortunately, no biopsies were performed in a DSA-negative control group in these studies, making it difficult to ascertain the precise odds of dnDSA to signal TCMR risk. Nonetheless, as discussed above, the association between TCMR and dnDSA development has been described previously in multiple studies. The study by Loupy et al. [57] seems to contrast this suggested association, as they showed that significantly more patients without DSA developed subclinical TCMR compared to patients with DSA. However, the majority of patients with DSA in this study had preformed DSA, not dnDSA. This was also reflected in patients with subclinical TCMR, as only 5 out of 17 (29%) of these patients had dnDSA. This could imply that there is no association between preformed DSA and TCMR, while there might be one for dnDSA and TCMR. Others were also not able to relate pretransplant DSA and TCMR development [84, 85]. However, these studies did not take into account the possible presence of mixed rejection in these analyses, or pooled these type of rejections with patients with ABMR. The study by Coemans et al. [78] did adjust their analysis accordingly and found that while pretransplant DSA was not associated with isolated TCMR, it was associated with total TCMR including mixed rejections. Nevertheless, the results of these studies might be further evidence for the previously described view on rejection as a spectrum of different clinical and histological manifestations. These may occur in sequence, as TCMR can result in dnDSA development, which can lead to ABMR. In contrast, preformed DSA may not necessarily lead to development of isolated TCMR. Collectively, these results imply that a biopsy serves to diagnose latent rejection (ABMR, TCMR or mixed rejection) in around half of patients with subclinical DSA, which is in line with previous recommendations on performing an allograft biopsy these patients [15]. While the number of papers warrants strong support for this statement, the evidence is mainly observational. This is reflected in the grading.
Upon Detection of a dnDSA, the Pathogenicity and the Impact on Prognosis is Currently Best Assessed by Doing a Biopsy (1C)
Prognostic Value of a Banff Classified Rejection Diagnosis
Aside from the diagnostic purposes of an allograft biopsy in patients with subclinical DSA, it may also have prognostic value in predicting allograft loss. As stated before, not all patients who develop DSA seem to lose their graft or even show declining allograft function. Wiebe et al. [22] showed that 50% of patients still had a functioning allograft 10 years post-detection of the subclinical dnDSA. Therefore, further risk stratification regarding the pathogenicity of these subclinical dnDSA seems necessary. The Banff classified rejection diagnosis in these patients may provide further risk-stratification for detrimental transplant outcomes. Multiple studies showed that KTR with subclinical DSA and histological evidence of ABMR had significantly worse allograft survival rates and allograft functional decline than those without histopathological rejection at light microscopy [30, 57, 77, 78, 86]. Others show a similar trend, albeit not statistically significant [79, 82]. Moreover, Bertrand et al. [77] and Loupy et al. [57] showed that patients with subclinical dnDSA but without ABMR had excellent 8 years allograft survival (>90%) and stable graft function. This suggests that the rejection diagnosis could be prognostically more important for graft outcome than the dnDSA status itself in patients without graft dysfunction. This was further corroborated by Parajuli et al. [87] in a cohort of 587 patients without rejection at an initial protocol or indication biopsy, whereafter there was no difference in 5 years allograft loss rates between DSA-positive and DSA-negative patients. Though, dnDSA positivity in patients with a negative index biopsy was associated with subsequent rejection.
Prognostic Value of Inflammation Activity
Beyond the prognostic value of the Banff classified rejection diagnosis in patients with subclinical DSA, the severity of the Banff recognized acute pathological lesions may perhaps offer further risk-stratification in patients with rejection. A prospective cohort study of 215 patients showed that while DSA were univariately associated with renal function decline, this was no longer statistically significant when analyzed with a multivariate model including MVI and tubulitis [88]. This suggests that the presence of histological markers may define a more severe phenotype in patients with DSA. Wiebe et al. [22] showed in multivariate analysis of a small subcohort of 23 subclinical patients with dnDSA that tubulitis was a strong predictor for allograft loss. Studies by De Kort et al. [89] and the iBox study by Loupy et al. [90] elegantly showed that increasing levels of MVI severity score in patients with DSA is independently associated with worse allograft survival. A more recent study on semi-supervised clustering through data-driven mathematic modeling by Vaulet et al. [91] further corroborated the prognostic value of inflammation activity as determinant of allograft loss within patients with DSA.
Prognostic Value of Chronicity Markers
Histological chronicity markers also impact allograft survival. The presence of transplant glomerulopathy is implicated as independent risk factor for allograft attrition in multivariate analysis by multiple studies [22, 78, 90, 92]. Other chronicity markers such as interstitial fibrosis or tubular atrophy also seem to independently infer risk for allograft loss in patients with DSA [90]. More recent research showed that patients with increasing chronicity scores as determined by an aggregate of several chronicity markers have significantly worse prognosis in terms of allograft survival [93]. A follow-up study by Vaulet et al. [94] validated these results, again through a semi-supervised clustering approach, and found that clusters with higher levels of chronicity were associated with increasingly higher rates of allograft loss. Importantly, they assessed the impact of time since transplant of the biopsy in this study. Even though there was an association with clustering based on chronicity, clustering solely based on time of biopsy could not discriminate in allograft loss rate. This indicated that pattern of chronicity scores was an independent risk factor for poor allograft survival, regardless of the post-transplant time of the biopsy.
Temporal Association Between Activity and Chronicity and Relation With Efficacy of Treatment
Even though activity and chronicity are viewed as separate entities for the sake of the analyses in these studies, it should not be forgotten that they are intertwined. The temporal association between aABMR and chronic lesions associated with cABMR such as transplant glomerulopathy, peritubular capillary basement membrane multilayering and transplant arteriopathy is well described in both preclinical models and clinical studies [57, 69, 70, 78, 95–97]. Previous research in patients with TCMR has shown that chronic scarring is a determinate for poor response to treatment [98, 99]. Haas et al. [100] has also previously shown that early intervention in patients with ABMR may prevent chronic lesions such as transplant glomerulopathy. Recently, Wu et al. [101] did not observe any effect of current treatment options in patients with chronic ABMR and transplant glomerulopathy further indicating that late stages are less responsive to therapy. It could thus be of interest to identify patients at an earlier stage of the ABMR disease process. If a latent phase with subclinical DSA is an earlier stage in the continuum of rejection, then a biopsy taken at this stage may theoretically show less chronicity and these patients could perhaps be more amendable to treatment. Unfortunately, very few studies investigated this. Parajuli et al. [102] found that the Banff sum chronicity and transplant glomerulopathy scores of patients with underlying ABMR at biopsy were significantly lower in subclinical ABMR compared to dysfunctioning allografts with ABMR. Additionally, Wiebe et al. [34] found that no patients with subclinical dnDSA had evidence of transplant glomerulopathy. However, more research is needed to confirm this hypothesis, as current data is insufficient to draw meaningful conclusions.
Timing of the Allograft Biopsy
While this body of evidence seems to point out the additional prognostic value and possible clinical utility of an allograft biopsy in patients with (subclinical) DSA, it does not necessarily provide direction on when to perform this biopsy within the subclinical stage. The study by Schinstock et al. [30] clearly showed that within dnDSA-positive patients with a negative index biopsy, a follow-up biopsy 1 year later yields significantly more positive cases of ABMR. This appears to contrast aforementioned studies which suggested that an initial negative biopsy infers significantly less risk in patients who have developed dnDSA. However, the findings by Schinstock et al. [30] could be explained by the fact that not all their included biopsies at either dnDSA detection or follow-up were in fact in a subclinical setting. This may affect the a priori probability of finding underlying rejection at follow-up. Alternatively, the worse prognosis of the minority group who do eventually develop rejection may have been masked by the majority who remained without significant graft injury in other studies. Nevertheless, Schinstock et al. [30] could indicate that performing the biopsy too early could lead to false negative findings. Whereas no histopathological rejection at light or electron microscopy might be visible in these cases, there may in fact still be rejection at the molecular level. Previous research has shown the independent prognostic value of molecular ABMR gene transcripts for allograft attrition within patients with Banff classified ABMR [103]. The INTERCOMEX study has shown the added clinical value of these molecular gene expression transcripts for identifying rejection [104]. Two studies on molecular gene transcript classifiers further show that DSA-positive patients who present with high levels of these classifiers but show no histopathologic evidence of ABMR at light microscopy have more risk to develop histologic ABMR at subsequent biopsies compared to patients with low molecular ABMR gene transcript levels [105, 106]. Molecular analysis may thus offer additional prognostic value in case of a microscopically negative index biopsy, however these techniques are not yet available in most centers and require further validation. Some clinicians could perhaps consequently conclude that upon dnDSA detection, a certain amount of time should elapse before a biopsy is conducted, as this may decrease the chance of a negative biopsy result in those patients with molecular but not yet microscopic histological rejection. However, this may negatively impact potential efficacy of treatment in patients who would have more chronicity on later biopsies. Additionally, aforementioned studies on biopsy results upon subclinical dnDSA detection clearly show rejection in approximately 50% of cases. These would all be detected later by postponing a biopsy. An alternative strategy could entail a follow-up biopsy, if the index biopsy is negative. No study has been conducted which specifically addresses and compares the impact of these strategies on transplant outcomes. Therefore, more research on the optimal time of biopsy in patients with subclinical DSA is needed. Nevertheless, the additional prognostic value of renal biopsy information on both the Banff recognized rejection diagnosis and of the severity of the pathological lesions in patients with subclinical DSA seems clear. Therefore, despite the mostly single-center observational evidence, we strongly recommend to perform an allograft biopsy to further determine the pathogenicity and impact of developed subclinical dnDSA, if prognostication is desired.
Efforts Should be Made to Standardize Testing and Reporting of DSA, Including Information on MFI, Their Plausibility and Possible Cross-Reactive Antigens/Epitopes (1B)
A prerequisite for any screening strategy is the availability of a suitable test system which is acceptable to the population and with facilities available for diagnosis and treatment. The SAB-SPI test is currently the test system of choice to define DSA. This method is semiquantitative, highly specific, sensitive and able to detect and identify anti-HLA antibodies. However, differences within and between laboratories impair reproducibility when it comes to the definition of DSA in both clinical practice and trials. A recent systematic review showed that the reporting of DSA in clinical trials had huge variability concerning assay type, DSA verification, MFI cutoff to define DSA and the prevention of prozone [107]. The level of “not reported” was determined at +/−15% for assay type, >30% for DSA verification and MFI cut off and around 80% for prozone treatment. Not only antibody tests have to be taken into account. Senev et al. [108] showed that 23% of DSA defined on a low resolution level could not be confirmed if correlated to second field high resolution HLA-typing results. Laboratory factors, as well as donor and patient factors, are inherent limitations to the testing and reporting of DSA [2, 3]. MFI values underestimate broad reacting specificities as Bw4/Bw6 or beads saturated with antibody. MFI does not reflect titer and one should bear in mind that SAB-SPI tests are qualitative, at best semiquantitative tests [42, 109]. Potential pitfalls notwithstanding, HLA-antibody detection and antigen/epitope specificity identification have never been as good as today. HLA-antibody assessment using solid phase assays including all major HLA-loci are already recommended in the 2017 North-American Sensitization in Transplantation: Assessment of Risk workgroup (STAR) report [109]. Initiatives such as the STAR workgroup [109, 110] are essential to clarify the expectations and limitations of current clinically used DSA detection methods. Clinicians need to receive comprehensive reports in a timely manner while being informed on the limitations of individual assays and results. Additionally, HLA-immunologists need to understand the clinical course of a patient after transplantation. Whereas HLA-labs are highly involved in the definition of acceptable antigens pretransplant, they are less involved in the posttransplant follow-up of individual patients. To increase clinical utility and validity, feedback should not only go from the lab to the clinic but also vice versa, resulting in both standardized analytical and clinical reporting. The following information can be helpful in DSA reporting: risk category of the patient at the moment of transplantation, DSA chronology, and the indication of DSA testing. This interaction is specifically needed to address the potential pitfalls of DSA screening in the entity of DSA-negative ABMR.
International standards for HLA-labs should focus on the different aspects that can interfere with the definition of DSA as a follow-up biomarker for subclinical DSA. These can include definition of MFI (Median, Mean, trimmed mean), signal-to-background calculation or plausibility evaluation.
Although the current SAB-SPI allow identification of DSA, further research is required to standardize DSA monitoring in patients with functioning grafts. The use of SAB-SPI methods measuring C3d or C1q complement fixing of DSA can have additional value but needs further validation and cannot currently be recommended as a biomarker for subclinical DSA monitoring, as conflicting retrospective studies exist [111, 112]. Conflicting studies also exist in regards to IgG subclass differentiation [55, 113]. The role of non-HLA post-transplant does not seem to be impactful, but the number of studies is currently limited [114].
Methods to detect B cell memory [115, 116] or to detect specific antibody parameters as affinity and avidity [117] are currently not available on a large scale nor are they ready as posttransplant monitoring biomarker. Further research on these topics is required.
Whilst Post-Transplant Monitoring of Preformed DSA in Patients With Stable Graft Function Might be Helpful, Additional Clinical and Laboratory Parameters Should Also be Considered When Deciding if a Biopsy Should be Performed. (2C)
Development of dnDSA could prompt clinicians to further investigate a patient for underlying pathology. Here, we consider monitoring patients with subclinical preformed DSA. We will not argue against the validity and prognostic value of a biopsy per se in these patients. However, it is more difficult to determine a prompt to biopsy in patients with preformed DSA. It could be argued that post-transplant persistence of preformed DSA could prompt a biopsy as some preformed antibodies may gradually disappear from the circulation. Previous studies indicate that persistence of preformed DSA infers a higher risk of allograft loss and rejection than DSA that have disappeared [118–123], though some contradict this conclusion [88, 124]. Additionally, studies comparing allograft loss in patients with cleared preformed DSA versus no preformed DSA give conflicting results [118, 120, 125]. Furthermore, no study has examined the predictive value of clearance of preformed DSA. Thus, it is currently uncertain whether grafts in patients with cleared preformed DSA have a survival disadvantage or suffer higher rates of rejection compared to grafts in regular non-sensitized patients. It is therefore uncertain if clearance of preformed DSA should preclude a biopsy in patients without graft dysfunction. There is currently little evidence that post-transplant change in MFI of preformed DSA in patients with stable grafts has any predictive value. Early rise in preformed DSA MFI was associated with ABMR development in older studies [126, 127]. However, more recent in-depth analysis by Philpott et al. [128] of post-transplant temporal evolution of DSA indicated that allograft survival was impacted by the speed of change in MFI, rather than eventual delta MFI during the first month. They showed that patients with modulating preformed DSA (i.e., a rise then subsequent fall of MFI) had significantly better allograft survival than patients with sustained levels of preformed DSA (i.e., rising MFI and followed by sustained or stable MFI). This would indicate that a random point measurement of DSA MFI level in the early post-transplant course would provide minimal predictive information. Preformed DSA with high delta MFI compared to pretransplant levels could still be DSA which is undergoing a modulating course, which appears to infer less risk than DSA which had a more stable course in MFI. In this study, biopsies were only performed in case of allograft dysfunction, so it is difficult to extrapolate these results to patients with stable graft function. Moreover, delta MFI should be interpreted with caution in the absence of other clinical parameters, considering that the inter-laboratory variation of MFI can be as high as 62% [129] Consensus guidelines of the STAR workgroup are in line with this notion, as they state that any increase of MFI less than 50% is likely to be meaningless in otherwise “relaxed” situations [109]. Furthermore, even if the results of Philpott et al. [128] could be extrapolated to subclinical patients, they would only support careful monitoring in the first month post-transplant, as allograft survival was dependent on the evolution of DSA in that month. Unfortunately, no studies analyzed associations between late evolution in preformed DSA MFI and transplant outcomes. This leads to the conclusion that, although patients with preformed DSA and stable grafts can have latent rejection, there is currently no evidence to support the notion that monitoring these DSA alone provides a prompt to initiate further investigation of the patient. Additional clinical and laboratory parameters should thus also be considered, before deciding upon a biopsy in patients with preformed DSA. The lack of robust evidence regarding this topic is reflected in the grading of this recommendation. Alternatively, these patients might benefit from strategies utilizing protocol biopsies [2, 130] or a combined screening strategy using additional non-invasive biomarkers of rejection. A separate workgroup within the TLJ3.0 platform will publish consensus statements on the clinical validity and utility of these biomarkers and these methods are therefore beyond the scope of this consensus report.
DSA MFI Levels or Complement Binding Ability (C1q, C4d, C3d) Should Not Influence Decision-Making Regarding Whether a Biopsy in Patients With Subclinical dnDSA Should be Performed. (2C)
Development of subclinical dnDSA may prompt further investigation of the patient, though it would be of interest to define other factors that would help stratify the risk of underlying graft pathology. This may prevent needless allograft biopsies in patients with subclinical dnDSA, considering that not all patients with dnDSA have recognizable ongoing ABMR at biopsy. Previous studies have shown that patients with ABMR more often have antibodies aimed at HLA class II, however this is also likely related to class II antibodies being the most commonly formed type. [22, 92, 131] Moreover, a recent large cohort study did not find any difference in the proportion of patients with HLA class I dnDSA who have underlying ABMR, as compared to class II dnDSA. [29] Additionally, dnDSA HLA-class specificity does not seem to be significantly associated with graft survival in multivariate analysis. [29, 131] This indicates there is not enough evidence to state that DSA HLA-class significantly attenuates the risk of a rejection diagnosis or the graft prognosis and therefore should not influence the decision to omit a biopsy in patients with subclinical dnDSA. Multiple studies have associated other DSA characteristics with worse outcomes, such as MFI level (sum of all DSA MFI or highest individual MFI) [22, 88, 132–136], certain IgG subclasses [55, 137, 138], or complement binding ability (C1q, C4d, C3d) [54]. However, most studies do not provide information on the negative predictive value of these characteristics, which would be the parameter of interest in deciding on whether to omit a biopsy. Prospective randomized studies are lacking and only a few studies investigated the predictive value of these DSA characteristics. Eskandary et al. [82] retrospectively studied 86 patients with subclinical DSA and associated highest MFI, sum of MFI and complement binding ability with underlying ABMR. However, the individual C-statistics were moderate at best for each characteristic (0.77, 0.75 and 0.65 respectively). Additionally, a combined model of maximum or sum of MFI and either C1q, C4d or C3d-positivity did not improve the predictive power of the base model of only MFI significantly. The authors found that while a higher MFI cutoff of >5000 or >10000 enjoyed a higher specificity for ABMR (0.86 and 0.99 for both MFI characteristics), the sensitivity drastically reduced from 0.82, 0,84 to 0.34, 0.43 and 0.30, 0.27 respectively. These MFI cutoffs subsequently result in low negative predictive value for ABMR in patients with subclinical dnDSA (MFI > 5000: 0.63, 0.67; MFI > 10000: 0.64, 0.65, for maximum MFI and sum of MFI, respectively). This indicates at least 30% of underlying ABMR would be missed by preclusion of a biopsy based on MFI cutoffs >5000 in subclinical patients. The fact that MFI values do not reflect the strength of the antibody titer might be an important cause of the poor correlation between MFI values and outcome [42, 109]. A recent study could not identify a relationship between MFI at first occurrence and outcome, only a profound >50% reduction of dnDSA MFI values was associated with better graft survival in a multivariate model [29]. Another study by Viglietti et al. [139] performed analyses with allograft loss as outcome in 186 patients with both subclinical and clinical DSA. They found an equally moderate C-statistic regarding maximum MFI in the total group of patients with post-transplant DSA (0.72). This was only marginally better in specifically dnDSA-positive patients (0.75). No analysis regarding specific MFI cut-offs was performed. While C1q-binding was found to significantly increase the fit of the base model, the numerical increase in C-statistic was a marginal 0.028 in dnDSA-positive patients (0.751–0.779) Interestingly, IgG3-positivity strongly increased the fit of the model with improvement of the C-statistic from 0.75 to 0.88. Yet this specific characteristic was predominately present in patients whose dnDSA were detected after development of allograft dysfunction. Only 2% of patients whose dnDSA were detected as a part of regular annual screening were IgG3-positive, yet 74% and 57% of these patients had ABMR at biopsy one and two years post-transplant respectively. These studies indicate that while some DSA characteristics such as higher MFI or IgG3 positivity might increase the likelihood of underlying pathology in dnDSA-positive patients with stable grafts, absence of these characteristics also definitely do not exclude it. Therefore, as robust supporting evidence is lacking, it seems that none of these studied DSA characteristics can be used reliably to preclude a biopsy in patients with subclinical DSA. We therefore currently do not recommend utilizing these DSA characteristics as an aid in deciding if a biopsy of patients with subclinical dnDSA should be performed.
We Recommend Optimization of Maintenance Therapy, Including Addressing Non-Adherence in Patients Who Develop Subclinical dnDSA. Additional Treatment Should Only be Considered After Performing an Allograft Biopsy. (1C)
Optimization of Maintenance Therapy
A crucial element of a screening program is whether proper treatment exists and whether there is consensus on whom to treat. Optimization of maintenance therapy, which includes promoting adherence, reducing exposure to secondary risk factors such as hypertension and maintaining appropriate calcineurin inhibitor trough levels, has been recommended in previous consensus statements for the treatment of ABMR and TCMR [15]. Moreover, the consensus on managing modifiable risk in transplantation (COMMIT) workgroup addressed non-adherence and underexposure to immunosuppression as pivotal risk factors for poor transplant outcomes [140]. The importance of adequate exposure has also previously been demonstrated in patients with DSA. Multiple studies showed that DSA-positive patients with adequate exposure have better graft survival compared to DSA-positive patients who remain non-adherent or with iatrogenic underexposure to immunosuppression [22–24]. Development of dnDSA has been heavily correlated to underexposure to immunosuppression [22–28]. This risk factor for poor transplant outcomes can be addressed and this could be done irrespective of underlying histology, because dnDSA may still signal underexposure even if there is no microscopically visible rejection. However, the recently published OuTSMART trial, which analyzed the effects of optimization of maintenance therapy based on DSA monitoring results, seems to contradict these previous retrospective studies [21]. No significant difference was found in regards to graft survival between standard of care and optimization of maintenance therapy based on DSA monitoring. This randomized controlled trial (RCT) is qualitatively better evidence than observational research. However, it should be noted that the consenting participants in OuTSMART were already highly adherent at baseline. This is reflected by the low dnDSA incidence rate of 1.6% per year and may relate to the possibility of healthy survivor bias due to cross-sectional inclusion. Even though adherence improved significantly to even greater levels, it is uncertain whether it was to be expected that this should have resulted in improved graft survival. Nonetheless, this study does appear to show that broadening the immunosuppressive regimen does not have the expected effect on graft survival. Even the sensitivity analysis, which only included patients who were optimized to a triple therapy regime upon detection of dnDSA could not demonstrate survival benefit, though the confidence interval included both estimates of highly protective as well as highly hazardous effects. This could have been related to less allograft failure in DSA-positive patients than initially expected. Interestingly, total amount of biopsy-proven rejections was significantly lower in patients in the intervention arm, indicating that increased exposure does have immunological effect. Perhaps more benefit could be demonstrated if optimization of maintenance therapy is accompanied with biopsy-guided anti-rejection treatments as subclinical rejection was likely present in only 50% of subjects. More research in terms of broadening immunosuppressive regimen as a means of optimization of maintenance therapy is thus required for this to be recommended. Nevertheless, addressing non-adherence and secondary risk factors for progression are still important aspects of treatment, which we still strongly recommend in case of development of subclinical dnDSA. The ultimate goal is to optimize graft survival which includes taking into account competing mortality risk from infections, malignancies, and other toxicities.
Maintenance Immunosuppressive Target Levels
When subclinical donor-specific antibodies emerge, it becomes crucial to detect potential non-adherence and optimize the maintenance immunosuppressive regimen, unless there are contraindications present. In case of signs of ongoing alloimmunity, the convention in many center is often to switch to triple therapy with tacrolimus, mycophenolate analogues and maintenance steroids balanced against toxic side effects. Unfortunately, there is a current lack of strong evidence for exposure targets in kidney transplant recipients with subclinical dnDSA. To give some clinical directions, target tacrolimus exposure could be extrapolated from trough levels to prevent (additional) DSA [25, 28] rejection [141], and to improve graft survival [142–144]. Collectively, these studies suggest that maintaining the tacrolimus trough level between 5 and 8 ng/mL, which is in line with international recommendations, might prevent alloimmunity and optimize survival, albeit two studies suggested a potential lower threshold of 4 ng/mL in patients with very low intrapatient variability [141, 142]. However, whether this target range is helpful once caABMR ensues remains unknown. A study by Sablik et al. [145] did not find any survival difference between a tacrolimus trough greater or lesser than 5.9 ng/mL. Interestingly, they did find that higher intrapatient variability was significantly associated with poorer survival in patients with caABMR, suggesting that adherence and time in therapeutic range are probably more important exposure variables than attained trough levels within current clinical practice. Even less evidence is available regarding optimal mycophenolate exposure. A small single study found a trough >1.3 mg/L to prevent DSA formation [146]. It is reasonable to hypothesize that a clear exposure-relationship curve between mycophenolate and antibody formation might exist, considering the almost linear relation between MPA exposure and SARS-CoV-2 antibody formation [147]. No evidence is available for reintroduction of low-dose steroids, it is however often assumed that the anti-inflammatory effects and the diminished chance of acute rejection from maintenance steroids might have beneficial effects in the long-term but need careful balancing against side-effects [148]. Some evidence has emerged regarding the effectiveness of conversion from a CNI based immunosuppressive regime to costimulation blockade with belatacept [149]. Perhaps optimization of maintenance therapy could entail such a strategy, as it would effectively eliminate occult non-adherence due to the necessity of intravenous administration. Additionally, belatacept’s immunological mode of action may be more fitted for patients who have already developed a dnDSA as it interrupts T-follicular helper cell—B-cell interaction and could thus decrease B-cell stimulation and further reduce the evolution of DSA formation [29, 150]. Some studies have shown effectiveness of belatacept on DSA levels and on the (lower) incidence of ABMR in sensitized patients [149–152]. Interestingly, DSA positivity was not associated with graft loss in a small cohort of patients converted to belatacept, though the presence of aABMR with MVI was independently associated with treatment failure [153]. It has to be noted however, that the incidence of TCMR was significantly increased, especially in patients converted within the first year post-transplant [154]. We therefore recommend more research to be conducted on the role of costimulation blockade as a means to optimize maintenance therapy in patients with subclinical DSA.
Pre-Emptive Treatment In Lieu of an Allograft Biopsy
In regards to further treatment of patients with subclinical dnDSA before conducting a biopsy, evidence is lacking. Only one small cohort study has been identified, in which patients with subclinical DSA were treated with bortezomib, PP, IVIG and corticosteroids without performing a biopsy to confirm rejection [155]. This study showed that patients who achieved DSA clearance had more stable 2 year allograft function compared to those with persistent DSA. However, no control group was included and thus it cannot be concluded that improvement in outcome was due to treatment. Furthermore, irrespective of efficacy, subjecting all patients with subclinical dnDSA to such a strong and broadly targeting immunosuppressive regimen might be difficult to justify, considering that roughly half of this population have no underlying observable histological injury [30, 57, 78, 80–83]. In addition, transient spontaneous negativity of dnDSA has been observed in 24% of patients with subclinical dnDSA and complete clearance of dnDSA has been observed in around 10% of patients [29]. Lastly, identification of the Banff classified type of rejection through a biopsy will ensure that patients with underlying cell-mediated rejection are not unnecessarily subjected to therapy aimed at antibodies and vice versa. We therefore do not recommend additional preemptive treatment of patients with subclinical dnDSA, besides optimization of maintenance therapy, without performing an additional allograft biopsy.
Treatment of Subclinical T-cell Mediated Rejection
Amongst dnDSA-positive patients with underlying rejection, those with subclinical TCMR may have the best evidence for gained benefit. Treatment of subclinical TCMR has been investigated in multiple studies (Table 5). A literature review by Mehta et al. [156] revealed that most available studies [157–161] at the time showed that subclinical acute TCMR (aTCMR) is associated with inferior outcomes. Choi et al. [162] observed significantly lower 10 years allograft survival in patients with untreated early subclinical TCMR vs. non-rejectors (62.3% vs. 96.2%). Consequently, ESOT advocates subclinical aTCMR to be considered as primary efficacy endpoints in clinical trials [163]. The first evidence of treatment came from a randomized trial by Rush et al. [161]. They showed that treatment of early subclinical TCMR detected in protocol biopsies leads to lower chronicity scores, less late rejections and more stable and lower creatinine levels at 2 years post-transplant than untreated patients. Another RCT by Kurtkoti et al. [160] showed similar results in regards to lower creatinine levels at 6 and 12 months. These older studies could be criticized for having been conducted before the tacrolimus era and thus being less applicable to current practice. A more recent randomized trial of early protocol biopsy and treatment of subclinical TCMR in patients with tacrolimus and mycophenolate analogues showed no benefit of treatment [164]. There was no difference in renal function at 6 months and chronic histology scores were in fact higher in the treatment arm. This study was, however, limited by the relatively low frequency of subclinical rejection at early protocol biopsy, as only 4.6% showed subclinical TCMR. Additionally, chronicity scores in the control arm appeared to improve from implantation to the 6 months biopsy in some patients with seemingly no additional intervention. This perhaps indicates other unknown factors may have influenced the results of this study and limits the potential conclusions that can be drawn from it. In terms of more recent observational research, Seifert et al. [165] analyzed protocol biopsies at 3 and/or 6 months in 120 pediatric patients. They showed that 13 treated patients with subclinical aTCMR still had a significantly increased risk of meeting the composite endpoint of death-censored allograft loss and acute rejection at 5 years post-transplant, compared to patients without rejection. However, choice of treatment modality of this low number of patients was at the discretion of the physician. In contrast, larger recent studies showed no significant difference in delta creatinine, odds of 50% eGFR loss, or allograft survival between subclinical TCMR patients treated standardly with pulse steroids and a control group without TCMR at protocol biopsy; [57, 166]. It should be noted that these studies were mainly performed in DSA-negative patients. Thus, less is known about treatment of DSA-positive subclinical TCMR cases, although there is a broad consensus about the detrimental long-term consequences on ongoing inflammation in renal allografts [163]. However, Cherukuri et al; [24] analyzed the effect of treatment with steroid pulses on patients with TCMR and/or DSA, although these were not specifically subclinical cases. Patients with underlying TCMR and no DSA had no significant risk of graft loss. However, TCMR with concurrent DSA was a significant risk factor for 4 years allograft attrition in multivariate analysis, even when treated. Crucially, this significant risk was attributable to non-adherence. Adherent and pulse steroid treated patients with DSA and TCMR had no increased risk of allograft loss compared to patients without DSA and rejection, whereas non-adherent, pulse steroid treated patients with DSA and TCMR had drastically lower graft survival rates. This seemingly indicates that DSA-positive patients with underlying TCMR may still be amendable to current treatment modalities, provided they are adherent. This further signals that strengthening adherence is an important treatment option and is recommended by us and others in patients with dnDSA [15, 140]. There are currently no guidelines on the treatment of subclinical TCMR [163]. A recent systematic review and meta-analysis by Ho et al. [167] showed through the included retrospective studies that most centers seem to treat subclinical TCMR (Banff 1a or higher) with pulse steroids and occasionally thymoglobulin. This is in line with two recent surveys, which show that more than 90% of North-American transplant centers have implemented pulse steroids or lymphocyte depleting antibodies as standard of care in these patients [168, 169]. Currently, ESOT is surveying this in Europe as well.
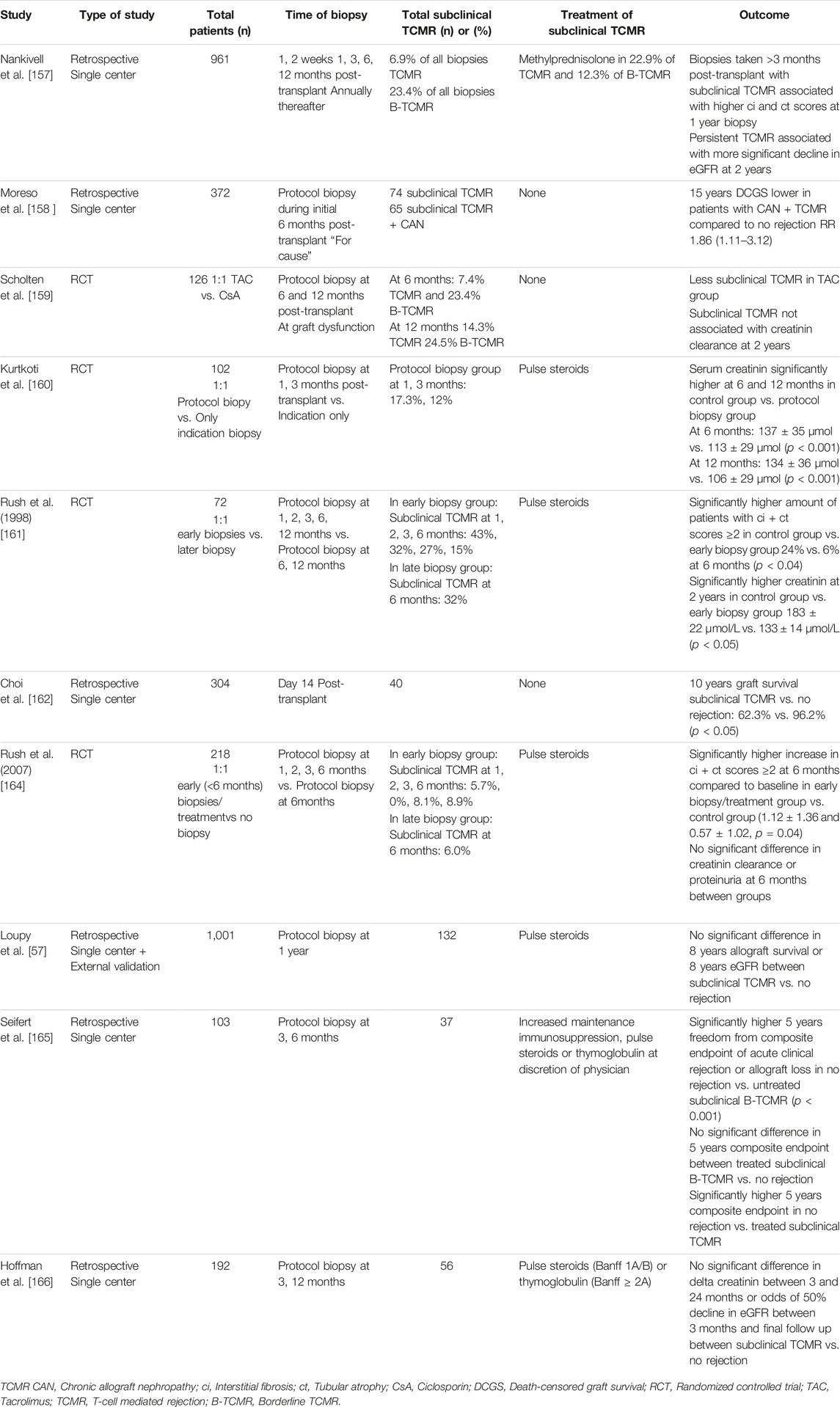
TABLE 5. Summary of studies on outcome of treated and untreated subclinical.
Treatment of Subclinical Antibody-Mediated Rejection
As a substantial amount (40%–50%) of patients with subclinical dnDSA will have signs of ABMR upon biopsy, it is important to review the evidence for treatment options in these patients. Recent consensus guidelines concluded that there is very little evidence for efficacy of current treatment protocols for ABMR in patients with dnDSA [15]. However, a retrospective study showed an incremental improvement in the treatment of ABMR; [170]. In addition, a small phase II prospective randomized trial with an IL-6 inhibitor has shown some promising results in chronic active ABMR (caABMR), and is currently being studied in a large multicenter phase III RCT [171, 172]. Additional evidence is emerging on the effectiveness of costimulation blockade, as discussed above, and anti-CD38 therapy in patients with aABMR and caABMR, the latter of which is currently being investigated in a phase II RCT in the form of felzartamab [149, 173]. In light of emerging data one may conclude that (early) acute ABMR with dnDSA (but without transplant glomerulopathy) could be more responsive to maintenance treatment optimization as well as PP and IVIG and eventually novel treatment regimens than patients with caABMR or cABMR, albeit all the treatment options have a low amount of supporting evidence. Active research in this area is ongoing and ABMR definition is becoming more precise [174]. Thus, there could potentially be benefit in finding and treating patients with early (subclinical) forms of ABMR before they present late with irreversible chronic lesions and clinical dysfunction. Some retrospective studies seem to support this hypothesis (Table 6). Parajuli et al. [102] showed similarly good post-biopsy allograft survival in patients with subclinical ABMR treated with IVIG and PP, as compared to protocol biopsied dnDSA-positive patients without rejection. Additionally, patients with treated subclinical ABMR had significantly better allograft survival than DSA-negative patients with indication biopsies or patients with treated clinical ABMR. Importantly, there was no difference in outcome between subclinical ABMR based on preformed DSA (type 1) vs. dnDSA (type 2). However, it must be noted that the post-biopsy follow-up time in patients with subclinical ABMR was relatively low at 31.0 ± 15.8 months. Orandi et al. [175] showed that patients with mostly type 1 subclinical ABMR treated by PP and in some situations rituximab or eculizumab had no significantly different rate of 5 years death-censored allograft loss compared to ABMR negative matched controls, whereas untreated patients had significantly more 5 years death-censored graft attrition rates compared to their control group. In addition, Yamamoto et al [79]. described some beneficial effects of PP and rituximab in 8 out of 18 (44%) of patients with subclinical type 2 ABMR whereby DSA levels reduced significantly or histological injury stabilized upon rebiopsy. In contrast, studies by Bertrand et al. [77] and Loupy et al. [57] found that allograft survival in treated subclinical ABMR patients was still significantly worse than patients without rejection. However, only 39% of patients with subclinical ABMR in the study by Loupy et al. [57] received specific treatment for subclinical ABMR and no analysis was performed comparing the treated and untreated group. It is apparent that more robust research on the effectiveness of treatment of subclinical ABMR is warranted. Nonetheless, the overall risk-benefit balance seems to be in favor of screening of DSA, which could result in early optimization of maintenance therapy. Moreover, further biopsy-guided treatment of subclinical TCMR and subclinical ABMR may be more effective than later treatment of clinical rejections, though evidence for this notion is more limited, as reflected in the grading of this recommendation.
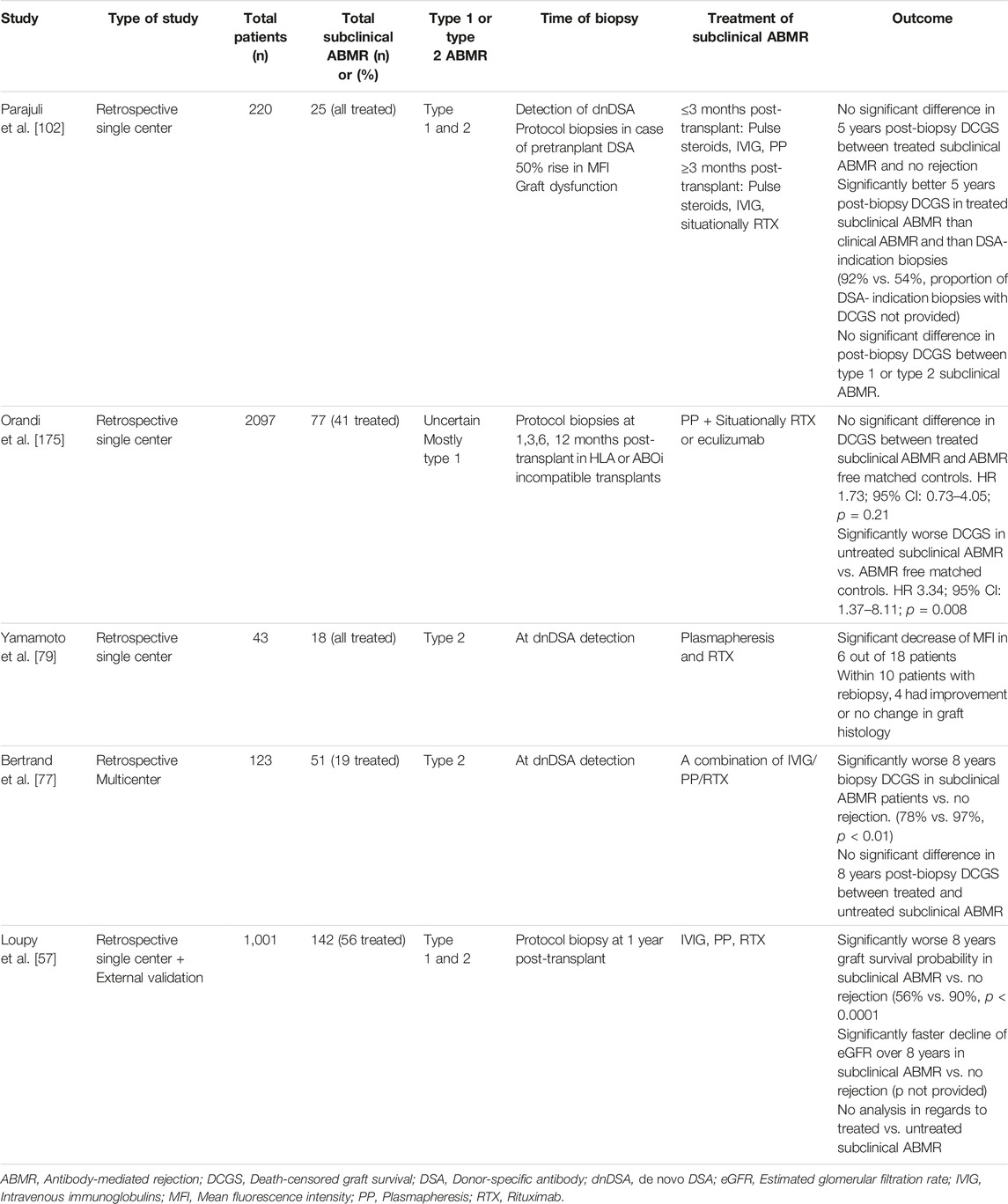
TABLE 6. Summary of studies on outcome of subclinical ABMR with or without treatment.
Cost-Effectiveness of DSA Monitoring in Patients With Stable Graft Function Will Depend on Incidence Rate of dnDSA and Importantly on Size Effect of Treatment (2D)
Assessment of the balance between medical risks and benefits of early case finding may determine that a screening program is medically justified, though this assessment does not necessarily determine whether it is cost-effective. As transplant centers have finite resources, DSA screening should be economically balanced to the cost of medical expenditure as a whole. Important aspects are the costs of the screening test and of the consequences of a missed case. The costs of a patient with graft loss due to ABMR who proceeds to renal replacement therapy far exceed the costs of those who retain their transplant by over €40.000 per year [176]. If one assumes that graft losses to ABMR account for around 1/3 of all graft losses [17] and takes into consideration the costs and benefits of potential treatment as well as morbidity and mortality rates of those treatments, then DSA screening seems justifiable on first glance. Unfortunately, evidence in the literature on this topic is very scarce. Kiberd et al. [177] performed a DSA monitoring cost-effectiveness modelling study. They found that costs per increased quality-adjusted life year (QALY) could range from $127.000 to $444.000, depending on the estimated efficacy of treatment and on the incidence rate of dnDSA. However, the model did not account for the fact that costs saved by not screening and treating early would still partly be spent later on treating patients when they do present with clinical dysfunction. This means that the presented costs per QALY are likely an overestimation, especially considering that most of the projected costs were attributed to the treatment of found cases, instead of DSA screening itself. Nonetheless, the basis for a cost-effective screening strategy is adequately illustrated through this modelling example. The only real-world data regarding cost-effectiveness comes from the previously mentioned OuTSMART study [21]. The incidence rate of dnDSA in this study population was lower than expected at 1.6% per year. This, in combination with no found benefit of optimization of maintenance therapy, resulted in a staggering incremental cost-effectiveness ratio of £1.692.222 per QALY for monitoring for DSA. As stated before, development of dnDSA pertains to multiple risk factors, and particularly to the immunological risk and epitope mismatch [4, 28, 46, 178]. The varied reported incidence rate in current literature likely attests to this, as some report a steady rate ranging from 1.5% to 5.4% per year in immunological low-risk patients [22, 179–181]. Others report increased incidence in the first year ranging from 3.2% to even 20% with a lower steady yearly rate thereafter ranging from 0.8% to 4.3% [30, 182, 183]. The lower incidence rate in OuTSMART could thus perhaps be a reflection of better organ allocation, better post-transplant overall care or it could simply reflect a different population in terms of age, healthy survivor bias from cross-sectional inclusion, ethnicity or proclivity to adhere to their medication as compared to the populations in the mentioned reports in the literature. Nonetheless, the results of this trial provide real-world validation of the modeling study by Kiberd et al. [177], as it shows that cost-effectiveness of DSA monitoring is dependent on the incidence rate of dnDSA and effect of treatment. Whether or not DSA monitoring is cost-effective, may thus in fact differ between centers, as incidence rate, local treatment protocols, and allograft biopsy strategy in case of subclinical dnDSA may differ. More trials, with standardized DSA definition and reporting, in various populations with additional allograft biopsies in case of subclinical dnDSA are ultimately needed to fully determine the cost-effectiveness of DSA monitoring.
Monitoring for dnDSA During Functional Graft Life Is a Continuous Process and Should Not Cease Upon Detection of dnDSA (2C)
Case-finding should be a continuing process and not a “once and for all” project. As new cases of subclinical rejection accumulate over time post-transplantation, DSA screening cannot be a one-time effort [29, 34]. The intensity and the longevity of the monitoring strategy should be reflected by the a priori chance of development of dnDSA over time. A recent large retrospective analysis shows that of 400 patients with dnDSA, 20% were found within the first year, 60% within 5 years and 85% within 10 years post-transplant, clearly indicating that even after 10 years post-transplant, patients may still develop dnDSA [29]. Unfortunately, as shown previously, the annual dnDSA incidence rate is not fully clear. Nevertheless, all studies indicate that dnDSA are constantly evolving and that the incidence does not reduce significantly after 1 year post-transplant. This subsequently implies that any time-limited monitoring strategy, although less costly, would be medically arbitrary and would miss new subclinical cases that occurred after screening ceased. The OuTSMART trial attests to this notion, as incidence rate did not diminish after a set amount of prospective monitoring years [21]. Another point of contention is whether monitoring should be continued for persistence or development of new dnDSA once a dnDSA has been detected. A retrospective study by DeVos et al. [184] found that patients with >60% positive DSA measurements in at least 3 separate assessments are more likely to progress to allograft loss than those with <60% positive measurements. López del Moral et al. [29] showed that dnDSA which eventually disappear, either temporarily or permanently, are associated with a lower rate of allograft loss than those who persist. Additionally, they showed that development of multiple dnDSA is associated with worse allograft survival, though this association was no longer statistically significant in multivariable analysis. In contrast, Kim et al. [88] found that resolved dnDSA was not associated with less decline in renal function. These studies, while somewhat conflicting, overall seem to suggest that newly developed dnDSA which eventually disappear are less likely to be associated with subsequent allograft loss. This implies that continued monitoring after dnDSA have already developed could serve important prognostic purposes. Moreover, additional dnDSA may develop, which could be cause for an additional allograft biopsy. Current low-grade evidence thus suggests that monitoring should not be discontinued after a set amount of post-transplant years, nor upon development of dnDSA.
The Optimal dnDSA Monitoring Scheme has Not Been Established, but a Routine Approach Would Be Antibody Monitoring at Three to Six Months Post-transplant and Annually Thereafter. (2C)
Another dilemma in regards to the continuing process of case finding entails the intensity of monitoring. In an ideal world, development of dnDSA would be noted immediately. But this would require a frequency of monitoring that is unlikely to be feasible. Centers which perform routine DSA monitoring seem to do so annually with one or more additional measurements in the first year post-transplant [30, 77, 80]. A more personalized approach could be monitoring intensity based on the immunological risk, this may also be more cost-efficacious, as lower risk patients could be subjected to less frequent screening. Monitoring intensity stratification based on HLA-matching might be easy to establish. Naturally, recipients of a completely HLA-identical donor kidney have no risk of developing HLA-DSA. Completely HLA-identical transplants are, however, rare. Most DSA appear to be aimed at HLA-DQ [185], though López del Moral et al. [29] showed that the proportion of patients with a full HLA-DQ match who developed dnDSA was comparable to those with a full HLA-B or HLA-DR match. This indicates that other HLA-loci mismatches should not so easily be disregarded. More recent evidence regarding molecular eplet HLA mismatching has emerged, whereby a low DQ/DR eplet mismatch was found to carry a negligible risk for development of DQ or DR dnDSA [26, 28]. In addition, analysis of the predictive value of the PIRCHEII and HLA-matchmaker molecular eplet mismatch algorithms showed that low eplet mismatch was associated with reduced probability of dnDSA development for both class I and II HLA-loci [186]. Lastly, post-hoc analysis of the CELLIMIN trial showed that high molecular eplet mismatch load was associated with development of dnDSA for both HLA-classes [187]. These studies indicate that low levels of total eplet mismatch load could be a reason to lower DSA monitoring intensity or even omit it. Personalized DSA monitoring intensity based on molecular mismatch thus seems promising. However, further validation of this risk-stratification technique in prospective trials on DSA screening is needed and more research is thus recommended. Currently, no study has been conducted which compares outcomes of different monitoring frequency strategies. Notwithstanding, the study by Parajuli et al [102] shows that patients with subclinical dnDSA who are detected, biopsied and treated through a strategy consisting of screening after 6 months and annually thereafter have good outcome. This suggests that more intensive monitoring may be unnecessary. Additionally, a monitoring interval greater than 1 year might be ill-advised, as studies in untreated subclinical ABMR show more chronic lesions within 1 year post-diagnosis [72, 97]. This may indicate that patients detected beyond 1 year from inception of the dnDSA may be more difficult to treat. Lastly, considering multiple studies have indicated increased incidence of development of dnDSA in the first year post-transplant, it might be advisable to perform an additional measurement within three to 6 months post-transplant [29, 30, 182, 183]. It thus appears from current low-level evidence that, until more robust immunological risk-stratification methods are validated, monitoring strategies consisting of screening within the first three to 6 months post-transplant and annually thereafter may seem pragmatic. However, more prospective research is needed to determine the optimal monitoring strategy.
Summary and Next Steps
The authors suggest that, based on current available evidence and the assessment of each individual Wilson & Jungner criterium, monitoring for development of dnDSA has clinical utility to further optimize long-term graft survival. A routine approach for such a strategy could be annual monitoring with an additional assessment within the first three to 6 months post-transplant. Monitoring should not cease after a certain amount of time or after dnDSA has already developed. Subclinical dnDSA development should lead to promotion of adherence and addressment of secondary risk factors. Further treatment should only be considered after performing an allograft biopsy to diagnose underlying rejection. Evidence for further treatment guided by such biopsies in subclinical patients is limited. However, certain patients with early rejection may respond to it empirically and treatment of subclinical TCMR has become standard of care in most centers. Novel treatments may provide additional efficacy in terms of prolonging allograft survival in the near future. Ultimately, further prospective trials are necessary to fully determine the benefits of such treatment strategies and their cost-effectiveness. Monitoring preformed DSA and their evolution in the subclinical setting post-transplantation with currently available validated assays may not provide a clear enough signal for possible underlying pathology. Additional clinical and laboratory parameters should therefore be considered before deciding to perform a biopsy in these patients. However, this does not preclude DSA monitoring in these patients, as development of additional dnDSA should equally lead to further investigation and treatment of these individuals.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
Involved in the conception or design of the work: DB, SM, KB, CL, EC, DB, CM, AD, M-PE, MN, and AV. Literature screen and review: DB, SM, KB, CL, EC, DB, CM, AD, M-PE, MN, and AV. Drafted the article: DB, SM, KB, CL, EC, DB, CM, AD, M-PE, MN, and AV. Critically revised the article: DB, SM, KB, CL, EC, DB, CM, AD, M-PE, MN, and AV. Finally approved the version to be published: DB, SM, KB, CL, EC, DB, CM, AD, M-PE, MN, and AV. All authors contributed to the article and approved the submitted version.
Group Members of Workgroup Composition
The ESOT workgroup subclinical DSA monitoring comprised of all main authors, as well as the following panel of independent experts: David Cucchiari, Lucrezia Furian, Giuseppe Ietto, Georgios Liapis, Lorna Marson, Mikhail Nozdrin, Michele Rossini, Stella Stabouli, Jelena Stojanovic, Stathis Tsiakas, Oleksei Voroniak, Angeliki Vittoraki, Gianluigi Zaza.
Funding
All costs related to taskforce and workgroup meetings were covered by ESOT, without external funding.
Conflict of Interest
KB declares honoraria and or travel support from: Aicuris, Astellas, Astra, CareDx, Carealytics Digital Health, Chiesi, MSD, Neovii, Natera, Paladin, Stada, Takeda, Veloxis, Vifor. AVR received lecture and consultancy fees from Sandoz, Chiesi, Astellas, Hansa, CSL Behring, and Novartis in the past three years, all of which went to his employer and none to personal bank accounts.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This manuscript and the ESOT Consensus Workgroup is a collaborative work product of ESOT and its Sections and Committees. We would like to thank Devi Mey, Justyna Klimek, Irene Garcia, Giovanna Rossi, Daniele Roppolo and the entire ESOT staff for their tireless efforts to support this endeavor. The authors also thank Liset Pengel and her coworkers at the Centre for Evidence in Transplantation, who provided the literature list based upon our drafted PICOs.
Abbreviations
aABMR, Active antibody mediated rejection; ABMR, Antibody mediated rejection; aTCMR, Acute T-cell mediated rejection; caABMR, Chronic active antibody mediated rejection; cABMR, Chronic antibody mediated rejection; CDC, Complement-dependent cytotoxicity assay; COMMIT, Consensus On Managing Modifiable risk In Transplantation workgroup; CTS, Collaborative Transplant Study; dnDSA, de novo donor-specific antibody; DSA, Donor-specific antibody; eGFR, Estimated glomerular filtration rate; ESOT, European Society for Organ Transplantation; GRADE, Grades of Recommendation Assessment, Development and Evaluation; HLA, Human leukocyte antigen; IgG, Immunoglobulin G; IVIG, Intravenous Immunoglobulins; KTR, Kidney transplant recipients; MFI, Mean fluorescence intensity; MHC, Major histocompatibility complex; MVI, Microvascular inflammation; PP, Plasmapheresis; TCMR, T-cell mediated rejection; TLJ, Transplantation Learning Journey; RCT, Randomized controlled trial; SPI, Solid phase immunoassay; STAR, North-American Sensitization in Transplantation: Assessment of Risk workgroup; Subclinical DSA, Donor-specific antibody that has been noted in patients who otherwise do not show any sign of clinical dysfunction of the allograft, such as significantly increased proteinuria or decreased eGFR; QALY, Quality-adjusted life year.
References
1. Patel, R, and Terasaki, PI. Significance of the Positive Crossmatch Test in Kidney Transplantation. N Engl J Med (1969) 280(14):735–9. doi:10.1056/NEJM196904032801401
2. Tait, BD, Susal, C, Gebel, HM, Nickerson, PW, Zachary, AA, Claas, FH, et al. Consensus Guidelines on the Testing and Clinical Management Issues Associated with HLA and Non-HLA Antibodies in Transplantation. Transplantation (2013) 95(1):19–47. doi:10.1097/TP.0b013e31827a19cc
3. Ziemann, M, Suwelack, B, Banas, B, Budde, K, Einecke, G, Hauser, I, et al. Determination of Unacceptable HLA Antigen Mismatches in Kidney Transplant Recipients. HLA (2022) 100(1):3–17. doi:10.1111/tan.14521
4. Bestard, O, Thaunat, O, Bellini, MI, Bohmig, GA, Budde, K, Claas, F, et al. Alloimmune Risk Stratification for Kidney Transplant Rejection. Transpl Int (2022) 35:10138. doi:10.3389/ti.2022.10138
5. Loupy, A, Haas, M, Roufosse, C, Naesens, M, Adam, B, Afrouzian, M, et al. The Banff 2019 Kidney Meeting Report (I): Updates on and Clarification of Criteria for T Cell- and Antibody-Mediated Rejection. Am J Transpl (2020) 20(9):2318–31. doi:10.1111/ajt.15898
6. Schinstock, CA, Askar, M, Bagnasco, SM, Batal, I, Bow, L, Budde, K, et al. A 2020 Banff Antibody-mediatedInjury Working Group Examination of International Practices for Diagnosing Antibody-mediated Rejection in Kidney Transplantation – a Cohort Study. Transpl Int (2020) 34(3):488–98. doi:10.1111/tri.13813
7. Wilson, JMG, and Jungner, GWorld Health Organization. The Principles and Practice of Screening for Disease. World Health Organization (1966). Available from: https://apps.who.int/iris/handle/10665/208882.
8. Cillo, U, Weissenbacher, A, Pengel, L, Jochmans, I, Roppolo, D, Amarelli, C, et al. ESOT Consensus Platform for Organ Transplantation: Setting the Stage for a Rigorous, Regularly Updated Development Process. Transpl Int (2022) 35:10915. doi:10.3389/ti.2022.10915
9. Hariharan, S, Israni, AK, and Danovitch, G. Long-Term Survival after Kidney Transplantation. N Engl J Med (2021) 385(8):729–43. doi:10.1056/NEJMra2014530
10. Coemans, M, Susal, C, Dohler, B, Anglicheau, D, Giral, M, Bestard, O, et al. Analyses of the Short- and Long-Term Graft Survival after Kidney Transplantation in Europe between 1986 and 2015. Kidney Int (2018) 94(5):964–73. doi:10.1016/j.kint.2018.05.018
11. Coemans, M, Callemeyn, J, and Naesens, M. Long-Term Survival after Kidney Transplantation. N Engl J Med (2022) 386(5):497–8. doi:10.1056/NEJMc2115207
12. Loupy, A, and Lefaucheur, C. Antibody-Mediated Rejection of Solid-Organ Allografts. N Engl J Med (2018) 379(12):1150–60. doi:10.1056/NEJMra1802677
13. Sellares, J, de Freitas, DG, Mengel, M, Reeve, J, Einecke, G, Sis, B, et al. Understanding the Causes of Kidney Transplant Failure: the Dominant Role of Antibody-Mediated Rejection and Nonadherence. Am J Transpl (2012) 12(2):388–99. doi:10.1111/j.1600-6143.2011.03840.x
14. Gaston, RS, Cecka, JM, Kasiske, BL, Fieberg, AM, Leduc, R, Cosio, FC, et al. Evidence for Antibody-Mediated Injury as a Major Determinant of Late Kidney Allograft Failure. Transplantation (2010) 90(1):68–74. doi:10.1097/TP.0b013e3181e065de
15. Schinstock, CA, Mannon, RB, Budde, K, Chong, AS, Haas, M, Knechtle, S, et al. Recommended Treatment for Antibody-Mediated Rejection after Kidney Transplantation: The 2019 Expert Consensus from the Transplantion Society Working Group. Transplantation (2020) 104(5):911–22. doi:10.1097/TP.0000000000003095
16. Djamali, A, Kaufman, DB, Ellis, TM, Zhong, W, Matas, A, and Samaniego, M. Diagnosis and Management of Antibody-Mediated Rejection: Current Status and Novel Approaches. Am J Transpl (2014) 14(2):255–71. doi:10.1111/ajt.12589
17. Mayrdorfer, M, Liefeldt, L, Wu, K, Rudolph, B, Zhang, Q, Friedersdorff, F, et al. Exploring the Complexity of Death-Censored Kidney Allograft Failure. J Am Soc Nephrol (2021) 32(6):1513–26. doi:10.1681/ASN.2020081215
18. Mohan, S, Palanisamy, A, Tsapepas, D, Tanriover, B, Crew, RJ, Dube, G, et al. Donor-specific Antibodies Adversely Affect Kidney Allograft Outcomes. J Am Soc Nephrol (2012) 23(12):2061–71. doi:10.1681/ASN.2012070664
19. Susal, C. Collaborative Transplant Study Newsletter 2 (2020). Available from: https://www.ctstransplant.org/public/newsletters/2020/2020-2.html?ts=3236805466841606 (Accessed February 28, 2023).
20. Sharma, A, Lewis, JR, Lim, WH, Palmer, S, Strippoli, G, Chapman, JR, et al. Renal Transplant Outcomes and De Novo Donor-specific Anti-human Leukocyte Antigen Antibodies: a Systematic Review. Nephrol Dial Transpl (2018) 33(8):1472–80. doi:10.1093/ndt/gfy077
21. Stringer, D, Gardner, L, Shaw, O, Clarke, B, Briggs, D, Worthington, J, et al. Optimized Immunosuppression to Prevent Graft Failure in Renal Transplant Recipients with HLA Antibodies (OuTSMART): a Randomised Controlled Trial. EClinicalMedicine (2023) 56:101819. doi:10.1016/j.eclinm.2022.101819
22. Wiebe, C, Gibson, IW, Blydt-Hansen, TD, Pochinco, D, Birk, PE, Ho, J, et al. Rates and Determinants of Progression to Graft Failure in Kidney Allograft Recipients with De Novo Donor-specific Antibody. Am J Transpl (2015) 15(11):2921–30. doi:10.1111/ajt.13347
23. Schinstock, CA, Dadhania, DM, Everly, MJ, Smith, B, Gandhi, M, Farkash, E, et al. Factors at De Novo Donor-specific Antibody Initial Detection Associated with Allograft Loss: a Multicenter Study. Transpl Int (2019) 32(5):502–15. doi:10.1111/tri.13395
24. Cherukuri, A, Mehta, R, Sharma, A, Sood, P, Zeevi, A, Tevar, AD, et al. Post-Transplant Donor Specific Antibody Is Associated with Poor Kidney Transplant Outcomes Only when Combined with Both T-Cell-Mediated Rejection and Non-adherence. Kidney Int (2019) 96(1):202–13. doi:10.1016/j.kint.2019.01.033
25. Davis, S, Gralla, J, Klem, P, Tong, S, Wedermyer, G, Freed, B, et al. Lower Tacrolimus Exposure and Time in Therapeutic Range Increase the Risk of De Novo Donor-specific Antibodies in the First Year of Kidney Transplantation. Am J Transpl (2018) 18(4):907–15. doi:10.1111/ajt.14504
26. Davis, S, Wiebe, C, Campbell, K, Anobile, C, Aubrey, M, Stites, E, et al. Adequate Tacrolimus Exposure Modulates the Impact of HLA Class II Molecular Mismatch: a Validation Study in an American Cohort. Am J Transpl (2021) 21(1):322–8. doi:10.1111/ajt.16290
27. Jung, HY, Kim, SH, Seo, MY, Cho, SY, Yang, Y, Choi, JY, et al. Characteristics and Clinical Significance of De Novo Donor-specific Anti-HLA Antibodies after Kidney Transplantation. J Korean Med Sci (2018) 33(34):e217. doi:10.3346/jkms.2018.33.e217
28. Wiebe, C, Rush, DN, Nevins, TE, Birk, PE, Blydt-Hansen, T, Gibson, IW, et al. Class II Eplet Mismatch Modulates Tacrolimus Trough Levels Required to Prevent Donor-specific Antibody Development. J Am Soc Nephrol (2017) 28(11):3353–62. doi:10.1681/ASN.2017030287
29. Lopez Del Moral, C, Wu, K, Naik, M, Osmanodja, B, Akifova, A, Lachmann, N, et al. The Natural History of De Novo Donor-specific HLA Antibodies after Kidney Transplantation. Front Med (Lausanne) (2022) 9:943502. doi:10.3389/fmed.2022.943502
30. Schinstock, CA, Cosio, F, Cheungpasitporn, W, Dadhania, DM, Everly, MJ, Samaniego-Picota, MD, et al. The Value of Protocol Biopsies to Identify Patients with De Novo Donor-specific Antibody at High Risk for Allograft Loss. Am J Transplant (2017) 17(6):1574–84. doi:10.1111/ajt.14161
31. Senev, A, Coemans, M, Lerut, E, Van Sandt, V, Kerkhofs, J, Daniels, L, et al. Eplet Mismatch Load and De Novo Occurrence of Donor-specific Anti-HLA Antibodies, Rejection, and Graft Failure after Kidney Transplantation: An Observational Cohort Study. J Am Soc Nephrol (2020) 31(9):2193–204. doi:10.1681/ASN.2020010019
32. Chemouny, JM, Suberbielle, C, Rabant, M, Zuber, J, Alyanakian, MA, Lebreton, X, et al. De Novo Donor-Specific Human Leukocyte Antigen Antibodies in Nonsensitized Kidney Transplant Recipients after T Cell-Mediated Rejection. Transplantation (2015) 99(5):965–72. doi:10.1097/TP.0000000000000448
33. Wan, SS, Chadban, SJ, Watson, N, and Wyburn, K. Development and Outcomes of De Novo Donor-specific Antibodies in Low, Moderate, and High Immunological Risk Kidney Transplant Recipients. Am J Transpl (2020) 20(5):1351–64. doi:10.1111/ajt.15754
34. Wiebe, C, Gibson, IW, Blydt-Hansen, TD, Karpinski, M, Ho, J, Storsley, LJ, et al. Evolution and Clinical Pathologic Correlations of De Novo Donor-specific HLA Antibody post Kidney Transplant. Am J Transpl (2012) 12(5):1157–67. doi:10.1111/j.1600-6143.2012.04013.x
35. Everly, MJ, Briley, KP, Haisch, CE, Dieplinger, G, Bolin, P, Kendrick, SA, et al. Racial Differences in Incident De Novo Donor-specific Anti-HLA Antibody Among Primary Renal Allograft Recipients: Results from a Single center Cohort Study. Transpl Int (2017) 30(6):566–78. doi:10.1111/tri.12937
36. von Moos, S, Schalk, G, Mueller, TF, and Laube, G. Age-associated Decrease in De Novo Donor-specific Antibodies in Renal Transplant Recipients Reflects Changing Humoral Immunity. Immun Ageing (2019) 16:9. doi:10.1186/s12979-019-0149-8
37. Wiebe, C, and Nickerson, P. Posttransplant Monitoring of De Novo Human Leukocyte Antigen Donor-specific Antibodies in Kidney Transplantation. Curr Opin Organ Transpl (2013) 18(4):470–7. doi:10.1097/MOT.0b013e3283626149
38. Louis, K, Macedo, C, Lefaucheur, C, and Metes, D. Adaptive Immune Cell Responses as Therapeutic Targets in Antibody-Mediated Organ Rejection. Trends Mol Med (2022) 28(3):237–50. doi:10.1016/j.molmed.2022.01.002
39. Basu, S, and Dorling, A. Regulation of T- and B-Cell Interactions Determines the Clinical Phenotype Associated with Donor-specific Antibodies. Kidney Int (2022) 101(5):877–9. doi:10.1016/j.kint.2022.02.020
40. Callemeyn, J, Lamarthee, B, Koenig, A, Koshy, P, Thaunat, O, and Naesens, M. Allorecognition and the Spectrum of Kidney Transplant Rejection. Kidney Int (2022) 101(4):692–710. doi:10.1016/j.kint.2021.11.029
41. Lefaucheur, C, and Loupy, A. Antibody-Mediated Rejection of Solid-Organ Allografts. N Engl J Med (2018) 379(26):2580–2. doi:10.1056/NEJMc1813976
42. Tambur, AR, and Wiebe, C. HLA Diagnostics: Evaluating DSA Strength by Titration. Transplantation (2018) 102(1):S23–S30. doi:10.1097/TP.0000000000001817
43. Viglietti, D, Bouatou, Y, Kheav, VD, Aubert, O, Suberbielle-Boissel, C, Glotz, D, et al. Complement-binding Anti-HLA Antibodies Are Independent Predictors of Response to Treatment in Kidney Recipients with Antibody-Mediated Rejection. Kidney Int (2018) 94(4):773–87. doi:10.1016/j.kint.2018.03.015
44. Viglietti, D, Loupy, A, Aubert, O, Bestard, O, Duong Van Huyen, JP, Taupin, JL, et al. Dynamic Prognostic Score to Predict Kidney Allograft Survival in Patients with Antibody-Mediated Rejection. J Am Soc Nephrol (2018) 29(2):606–19. doi:10.1681/ASN.2017070749
45. Lefaucheur, C, Viglietti, D, Mangiola, M, Loupy, A, and Zeevi, A. From Humoral Theory to Performant Risk Stratification in Kidney Transplantation. J Immunol Res (2017) 2017:5201098. doi:10.1155/2017/5201098
46. Tambur, AR, Bestard, O, Campbell, P, Chong, AS, Barrio, MC, Ford, ML, et al. Sensitization in Transplantation: Assessment of Risk 2022 Working Group Meeting Report. Am J Transpl (2023) 23(1):133–49. doi:10.1016/j.ajt.2022.11.009
47. Bharadwaj, P, Shrestha, S, Pongracz, T, Concetta, C, Sharma, S, Le Moine, A, et al. Afucosylation of HLA-specific IgG1 as a Potential Predictor of Antibody Pathogenicity in Kidney Transplantation. Cell Rep Med (2022) 3(11):100818. doi:10.1016/j.xcrm.2022.100818
48. Pernin, V, Bec, N, Beyze, A, Bourgeois, A, Szwarc, I, Champion, C, et al. IgG3 Donor-specific Antibodies with a Proinflammatory Glycosylation Profile May Be Associated with the Risk of Antibody-Mediated Rejection after Kidney Transplantation. Am J Transpl (2022) 22(3):865–75. doi:10.1111/ajt.16904
49. Lion, J, Taflin, C, Cross, AR, Robledo-Sarmiento, M, Mariotto, E, Savenay, A, et al. HLA Class II Antibody Activation of Endothelial Cells Promotes Th17 and Disrupts Regulatory T Lymphocyte Expansion. Am J Transpl (2016) 16(5):1408–20. doi:10.1111/ajt.13644
50. Thomas, KA, Valenzuela, NM, and Reed, EF. The Perfect Storm: HLA Antibodies, Complement, FcγRs, and Endothelium in Transplant Rejection. Trends Mol Med (2015) 21(5):319–29. doi:10.1016/j.molmed.2015.02.004
51. Llaudo, I, Fribourg, M, Medof, ME, Conde, P, Ochando, J, and Heeger, PS. C5aR1 Regulates Migration of Suppressive Myeloid Cells Required for Costimulatory Blockade-Induced Murine Allograft Survival. Am J Transpl (2019) 19(3):633–45. doi:10.1111/ajt.15072
52. Valenzuela, NM, and Reed, EF. Antibody-mediated Rejection across Solid Organ Transplants: Manifestations, Mechanisms, and Therapies. J Clin Invest (2017) 127(7):2492–504. doi:10.1172/JCI90597
53. Louis, K, Fadakar, P, Macedo, C, Yamada, M, Lucas, M, Gu, X, et al. Concomitant Loss of Regulatory T and B Cells Is a Distinguishing Immune Feature of Antibody-Mediated Rejection in Kidney Transplantation. Kidney Int (2022) 101(5):1003–16. doi:10.1016/j.kint.2021.12.027
54. Bouquegneau, A, Loheac, C, Aubert, O, Bouatou, Y, Viglietti, D, Empana, JP, et al. Complement-activating Donor-specific Anti-HLA Antibodies and Solid Organ Transplant Survival: A Systematic Review and Meta-Analysis. Plos Med (2018) 15(5):e1002572. doi:10.1371/journal.pmed.1002572
55. Lefaucheur, C, Viglietti, D, Bentlejewski, C, Duong van Huyen, JP, Vernerey, D, Aubert, O, et al. IgG Donor-specific Anti-human HLA Antibody Subclasses and Kidney Allograft Antibody-Mediated Injury. J Am Soc Nephrol (2016) 27(1):293–304. doi:10.1681/ASN.2014111120
56. Jackson, AM, Kanaparthi, S, Burrell, BE, Lucas, DP, Vega, RM, Demetris, AJ, et al. IgG4 Donor-specific HLA Antibody Profile Is Associated with Subclinical Rejection in Stable Pediatric Liver Recipients. Am J Transpl (2020) 20(2):513–24. doi:10.1111/ajt.15621
57. Loupy, A, Vernerey, D, Tinel, C, Aubert, O, Duong van Huyen, JP, Rabant, M, et al. Subclinical Rejection Phenotypes at 1 Year Post-Transplant and Outcome of Kidney Allografts. J Am Soc Nephrol (2015) 26(7):1721–31. doi:10.1681/ASN.2014040399
58. Gosset, C, Viglietti, D, Rabant, M, Verine, J, Aubert, O, Glotz, D, et al. Circulating Donor-specific Anti-HLA Antibodies Are a Major Factor in Premature and Accelerated Allograft Fibrosis. Kidney Int (2017) 92(3):729–42. doi:10.1016/j.kint.2017.03.033
59. Mengel, M. Deconstructing Interstitial Fibrosis and Tubular Atrophy: a Step toward Precision Medicine in Renal Transplantation. Kidney Int (2017) 92(3):553–5. doi:10.1016/j.kint.2017.04.041
60. Cardinal, H, Dieude, M, Brassard, N, Qi, S, Patey, N, Soulez, M, et al. Antiperlecan Antibodies Are Novel Accelerators of Immune-Mediated Vascular Injury. Am J Transpl (2013) 13(4):861–74. doi:10.1111/ajt.12168
61. Dragun, D, Muller, DN, Brasen, JH, Fritsche, L, Nieminen-Kelha, M, Dechend, R, et al. Angiotensin II Type 1-receptor Activating Antibodies in Renal-Allograft Rejection. N Engl J Med (2005) 352(6):558–69. doi:10.1056/NEJMoa035717
62. Lefaucheur, C, Viglietti, D, Bouatou, Y, Philippe, A, Pievani, D, Aubert, O, et al. Non-HLA Agonistic Anti-angiotensin II Type 1 Receptor Antibodies Induce a Distinctive Phenotype of Antibody-Mediated Rejection in Kidney Transplant Recipients. Kidney Int (2019) 96(1):189–201. doi:10.1016/j.kint.2019.01.030
63. Pineda, S, Sigdel, TK, Chen, J, Jackson, AM, Sirota, M, and Sarwal, MM. Novel Non-histocompatibility Antigen Mismatched Variants Improve the Ability to Predict Antibody-Mediated Rejection Risk in Kidney Transplant. Front Immunol (2017) 8:1687. doi:10.3389/fimmu.2017.01687
64. Callemeyn, J, Senev, A, Coemans, M, Lerut, E, Sprangers, B, Kuypers, D, et al. Missing Self-Induced Microvascular Rejection of Kidney Allografts: A Population-Based Study. J Am Soc Nephrol (2021) 32(8):2070–82. doi:10.1681/ASN.2020111558
65. Koenig, A, Chen, CC, Marcais, A, Barba, T, Mathias, V, Sicard, A, et al. Missing Self Triggers NK Cell-Mediated Chronic Vascular Rejection of Solid Organ Transplants. Nat Commun (2019) 10(1):5350. doi:10.1038/s41467-019-13113-5
66. Kitchens, WH, Chase, CM, Uehara, S, Cornell, LD, Colvin, RB, Russell, PS, et al. Macrophage Depletion Suppresses Cardiac Allograft Vasculopathy in Mice. Am J Transpl (2007) 7(12):2675–82. doi:10.1111/j.1600-6143.2007.01997.x
67. Qi, F, Adair, A, Ferenbach, D, Vass, DG, Mylonas, KJ, Kipari, T, et al. Depletion of Cells of Monocyte Lineage Prevents Loss of Renal Microvasculature in Murine Kidney Transplantation. Transplantation (2008) 86(9):1267–74. doi:10.1097/TP.0b013e318188d433
68. Schinstock, CA, Sapir-Pichhadze, R, Naesens, M, Batal, I, Bagnasco, S, Bow, L, et al. Banff Survey on Antibody-Mediated Rejection Clinical Practices in Kidney Transplantation: Diagnostic Misinterpretation Has Potential Therapeutic Implications. Am J Transpl (2019) 19(1):123–31. doi:10.1111/ajt.14979
69. Smith, RN, Kawai, T, Boskovic, S, Nadazdin, O, Sachs, DH, Cosimi, AB, et al. Chronic Antibody Mediated Rejection of Renal Allografts: Pathological, Serological and Immunologic Features in Nonhuman Primates. Am J Transpl (2006) 6(8):1790–8. doi:10.1111/j.1600-6143.2006.01351.x
70. Smith, RN, Kawai, T, Boskovic, S, Nadazdin, O, Sachs, DH, Cosimi, AB, et al. Four Stages and Lack of Stable Accommodation in Chronic Alloantibody-Mediated Renal Allograft Rejection in Cynomolgus Monkeys. Am J Transpl (2008) 8(8):1662–72. doi:10.1111/j.1600-6143.2008.02303.x
71. Loupy, A, Hill, GS, Suberbielle, C, Charron, D, Anglicheau, D, Zuber, J, et al. Significance of C4d Banff Scores in Early Protocol Biopsies of Kidney Transplant Recipients with Preformed Donor-specific Antibodies (DSA). Am J Transpl (2011) 11(1):56–65. doi:10.1111/j.1600-6143.2010.03364.x
72. Loupy, A, Suberbielle-Boissel, C, Hill, GS, Lefaucheur, C, Anglicheau, D, Zuber, J, et al. Outcome of Subclinical Antibody-Mediated Rejection in Kidney Transplant Recipients with Preformed Donor-specific Antibodies. Am J Transpl (2009) 9(11):2561–70. doi:10.1111/j.1600-6143.2009.02813.x
73. Loupy, A, Hill, GS, and Jordan, SC. The Impact of Donor-specific Anti-HLA Antibodies on Late Kidney Allograft Failure. Nat Rev Nephrol (2012) 8(6):348–57. doi:10.1038/nrneph.2012.81
74. Levine, DJ, Glanville, AR, Aboyoun, C, Belperio, J, Benden, C, Berry, GJ, et al. Antibody-mediated Rejection of the Lung: A Consensus Report of the International Society for Heart and Lung Transplantation. J Heart Lung Transpl (2016) 35(4):397–406. doi:10.1016/j.healun.2016.01.1223
75. O'Leary, JG, Cai, J, Freeman, R, Banuelos, N, Hart, B, Johnson, M, et al. Proposed Diagnostic Criteria for Chronic Antibody-Mediated Rejection in Liver Allografts. Am J Transpl (2016) 16(2):603–14. doi:10.1111/ajt.13476
76. Wu, GW, Kobashigawa, JA, Fishbein, MC, Patel, JK, Kittleson, MM, Reed, EF, et al. Asymptomatic Antibody-Mediated Rejection after Heart Transplantation Predicts Poor Outcomes. J Heart Lung Transpl (2009) 28(5):417–22. doi:10.1016/j.healun.2009.01.015
77. Bertrand, D, Gatault, P, Jaureguy, M, Garrouste, C, Sayegh, J, Bouvier, N, et al. Protocol Biopsies in Patients with Subclinical De Novo Donor-specific Antibodies after Kidney Transplantation: A Multicentric Study. Transplantation (2020) 104(8):1726–37. doi:10.1097/TP.0000000000003055
78. Coemans, M, Senev, A, Van Loon, E, Lerut, E, Sprangers, B, Kuypers, D, et al. The Evolution of Histological Changes Suggestive of Antibody-Mediated Injury, in the Presence and Absence of Donor-specific Anti-HLA Antibodies. Transpl Int (2021) 34(10):1824–36. doi:10.1111/tri.13964
79. Yamamoto, T, Watarai, Y, Takeda, A, Tsujita, M, Hiramitsu, T, Goto, N, et al. De Novo Anti-HLA DSA Characteristics and Subclinical Antibody-Mediated Kidney Allograft Injury. Transplantation (2016) 100(10):2194–202. doi:10.1097/TP.0000000000001012
80. Parajuli, S, Reville, PK, Ellis, TM, Djamali, A, and Mandelbrot, DA. Utility of Protocol Kidney Biopsies for De Novo Donor-specific Antibodies. Am J Transpl (2017) 17(12):3210–8. doi:10.1111/ajt.14466
81. Waldecker, CB, Zgoura, P, Seibert, FS, Gall, S, Schenker, P, Bauer, F, et al. Biopsy Findings after Detection of De Novo Donor-specific Antibodies in Renal Transplant Recipients: a Single center Experience. J Nephrol (2021) 34(6):2017–26. doi:10.1007/s40620-021-01040-y
82. Eskandary, F, Bond, G, Kozakowski, N, Regele, H, Marinova, L, Wahrmann, M, et al. Diagnostic Contribution of Donor-specific Antibody Characteristics to Uncover Late Silent Antibody-Mediated Rejection-Results of a Cross-Sectional Screening Study. Transplantation (2017) 101(3):631–41. doi:10.1097/TP.0000000000001195
83. Cornell, LD, Schinstock, CA, Gandhi, MJ, Kremers, WK, and Stegall, MD. Positive Crossmatch Kidney Transplant Recipients Treated with Eculizumab: Outcomes beyond 1 Year. Am J Transpl (2015) 15(5):1293–302. doi:10.1111/ajt.13168
84. Betjes, MGH, Sablik, KS, Otten, HG, Roelen, DL, Claas, FH, and de Weerd, A. Pretransplant Donor-specific Anti-HLA Antibodies and the Risk for Rejection-Related Graft Failure of Kidney Allografts. J Transpl (2020) 2020:5694670. doi:10.1155/2020/5694670
85. Frischknecht, L, Deng, Y, Wehmeier, C, de Rougemont, O, Villard, J, Ferrari-Lacraz, S, et al. The Impact of Pre-transplant Donor Specific Antibodies on the Outcome of Kidney Transplantation - Data from the Swiss Transplant Cohort Study. Front Immunol (2022) 13:1005790. doi:10.3389/fimmu.2022.1005790
86. Hayde, N, Broin, PO, Bao, Y, de Boccardo, G, Lubetzky, M, Ajaimy, M, et al. Increased Intragraft Rejection-Associated Gene Transcripts in Patients with Donor-specific Antibodies and normal Biopsies. Kidney Int (2014) 86(3):600–9. doi:10.1038/ki.2014.75
87. Parajuli, S, Joachim, E, Alagusundaramoorthy, S, Aziz, F, Blazel, J, Garg, N, et al. Donor-Specific Antibodies in the Absence of Rejection Are Not a Risk Factor for Allograft Failure. Kidney Int Rep (2019) 4(8):1057–65. doi:10.1016/j.ekir.2019.04.011
88. Kim, JJ, Balasubramanian, R, Michaelides, G, Wittenhagen, P, Sebire, NJ, Mamode, N, et al. The Clinical Spectrum of De Novo Donor-specific Antibodies in Pediatric Renal Transplant Recipients. Am J Transpl (2014) 14(10):2350–8. doi:10.1111/ajt.12859
89. de Kort, H, Willicombe, M, Brookes, P, Dominy, KM, Santos-Nunez, E, Galliford, JW, et al. Microcirculation Inflammation Associates with Outcome in Renal Transplant Patients with De Novo Donor-specific Antibodies. Am J Transpl (2013) 13(2):485–92. doi:10.1111/j.1600-6143.2012.04325.x
90. Loupy, A, Aubert, O, Orandi, BJ, Naesens, M, Bouatou, Y, Raynaud, M, et al. Prediction System for Risk of Allograft Loss in Patients Receiving Kidney Transplants: International Derivation and Validation Study. BMJ (2019) 366:l4923. doi:10.1136/bmj.l4923
91. Vaulet, T, Divard, G, Thaunat, O, Lerut, E, Senev, A, Aubert, O, et al. Data-driven Derivation and Validation of Novel Phenotypes for Acute Kidney Transplant Rejection Using Semi-supervised Clustering. J Am Soc Nephrol (2021) 32(5):1084–96. doi:10.1681/ASN.2020101418
92. Aubert, O, Loupy, A, Hidalgo, L, Duong van Huyen, JP, Higgins, S, Viglietti, D, et al. Antibody-Mediated Rejection Due to Preexisting versus De Novo Donor-specific Antibodies in Kidney Allograft Recipients. J Am Soc Nephrol (2017) 28(6):1912–23. doi:10.1681/ASN.2016070797
93. Haas, M, Mirocha, J, Huang, E, Najjar, R, Peng, A, Sethi, S, et al. A Banff-Based Histologic Chronicity index Is Associated with Graft Loss in Patients with a Kidney Transplant and Antibody-Mediated Rejection. Kidney Int (2022) 103:187–95. doi:10.1016/j.kint.2022.09.030
94. Vaulet, T, Divard, G, Thaunat, O, Koshy, P, Lerut, E, Senev, A, et al. Data-Driven Chronic Allograft Phenotypes: A Novel and Validated Complement for Histologic Assessment of Kidney Transplant Biopsies. J Am Soc Nephrol (2022) 33(11):2026–39. doi:10.1681/ASN.2022030290
95. Gloor, JM, Cosio, FG, Rea, DJ, Wadei, HM, Winters, JL, Moore, SB, et al. Histologic Findings One Year after Positive Crossmatch or ABO Blood Group Incompatible Living Donor Kidney Transplantation. Am J Transpl (2006) 6(8):1841–7. doi:10.1111/j.1600-6143.2006.01416.x
96. Haas, M. The Relationship between Pathologic Lesions of Active and Chronic Antibody-Mediated Rejection in Renal Allografts. Am J Transpl (2018) 18(12):2849–56. doi:10.1111/ajt.15088
97. Haas, M, Montgomery, RA, Segev, DL, Rahman, MH, Racusen, LC, Bagnasco, SM, et al. Subclinical Acute Antibody-Mediated Rejection in Positive Crossmatch Renal Allografts. Am J Transpl (2007) 7(3):576–85. doi:10.1111/j.1600-6143.2006.01657.x
98. Bouatou, Y, Viglietti, D, Pievani, D, Louis, K, Duong Van Huyen, JP, Rabant, M, et al. Response to Treatment and Long-Term Outcomes in Kidney Transplant Recipients with Acute T Cell-Mediated Rejection. Am J Transpl (2019) 19(7):1972–88. doi:10.1111/ajt.15299
99. Kwon, H, Kim, YH, Ko, Y, Lim, SJ, Jung, JH, Baek, CH, et al. Pure T-Cell Mediated Rejection Following Kidney Transplant According to Response to Treatment. PLoS One (2021) 16(9):e0256898. doi:10.1371/journal.pone.0256898
100. Haas, M, and Mirocha, J. Early Ultrastructural Changes in Renal Allografts: Correlation with Antibody-Mediated Rejection and Transplant Glomerulopathy. Am J Transpl (2011) 11(10):2123–31. doi:10.1111/j.1600-6143.2011.03647.x
101. Wu, K, Schmidt, D, Lopez Del Moral, C, Osmanodja, B, Lachmann, N, Halleck, F, et al. Poor Outcomes in Patients with Transplant Glomerulopathy Independent of Banff Categorization or Therapeutic Interventions. Front Med (Lausanne) (2022) 9:889648. doi:10.3389/fmed.2022.889648
102. Parajuli, S, Joachim, E, Alagusundaramoorthy, S, Blazel, J, Aziz, F, Garg, N, et al. Subclinical Antibody-Mediated Rejection after Kidney Transplantation: Treatment Outcomes. Transplantation (2019) 103(8):1722–9. doi:10.1097/TP.0000000000002566
103. Loupy, A, Lefaucheur, C, Vernerey, D, Chang, J, Hidalgo, LG, Beuscart, T, et al. Molecular Microscope Strategy to Improve Risk Stratification in Early Antibody-Mediated Kidney Allograft Rejection. J Am Soc Nephrol (2014) 25(10):2267–77. doi:10.1681/ASN.2013111149
104. Halloran, PF, Reeve, J, Akalin, E, Aubert, O, Bohmig, GA, Brennan, D, et al. Real Time Central Assessment of Kidney Transplant Indication Biopsies by Microarrays: The INTERCOMEX Study. Am J Transpl (2017) 17(11):2851–62. doi:10.1111/ajt.14329
105. Dominy, KM, Willicombe, M, Al Johani, T, Beckwith, H, Goodall, D, Brookes, P, et al. Molecular Assessment of C4d-Positive Renal Transplant Biopsies without Evidence of Rejection. Kidney Int Rep (2019) 4(1):148–58. doi:10.1016/j.ekir.2018.09.005
106. Madill-Thomsen, KS, Bohmig, GA, Bromberg, J, Einecke, G, Eskandary, F, Gupta, G, et al. Donor-Specific Antibody Is Associated with Increased Expression of Rejection Transcripts in Renal Transplant Biopsies Classified as No Rejection. J Am Soc Nephrol (2021) 32(11):2743–58. doi:10.1681/ASN.2021040433
107. Jatana, SS, Zhao, H, Bow, LM, Cozzi, E, Batal, I, Horak, T, et al. Seeking Standardized Definitions for HLA-Incompatible Kidney Transplants: A Systematic Review. Transplantation (2023) 107(1):231–53. doi:10.1097/TP.0000000000004262
108. Senev, A, Emonds, MP, Van Sandt, V, Lerut, E, Coemans, M, Sprangers, B, et al. Clinical Importance of Extended Second Field High-Resolution HLA Genotyping for Kidney Transplantation. Am J Transpl (2020) 20(12):3367–78. doi:10.1111/ajt.15938
109. Tambur, AR, Campbell, P, Claas, FH, Feng, S, Gebel, HM, Jackson, AM, et al. Sensitization in Transplantation: Assessment of Risk (STAR) 2017 Working Group Meeting Report. Am J Transpl (2018) 18(7):1604–14. doi:10.1111/ajt.14752
110. Tambur, AR, Campbell, P, Chong, AS, Feng, S, Ford, ML, Gebel, H, et al. Sensitization in Transplantation: Assessment of Risk (STAR) 2019 Working Group Meeting Report. Am J Transpl (2020) 20(10):2652–68. doi:10.1111/ajt.15937
111. Kamburova, EG, Wisse, BW, Joosten, I, Allebes, WA, van der Meer, A, Hilbrands, LB, et al. Pretransplant C3d-Fixing Donor-specific Anti-HLA Antibodies Are Not Associated with Increased Risk for Kidney Graft Failure. J Am Soc Nephrol (2018) 29(9):2279–85. doi:10.1681/ASN.2018020205
112. Loupy, A, Lefaucheur, C, Vernerey, D, Prugger, C, Duong van Huyen, JP, Mooney, N, et al. Complement-binding Anti-HLA Antibodies and Kidney-Allograft Survival. N Engl J Med (2013) 369(13):1215–26. doi:10.1056/NEJMoa1302506
113. Honger, G, Hopfer, H, Arnold, ML, Spriewald, BM, Schaub, S, and Amico, P. Pretransplant IgG Subclasses of Donor-specific Human Leukocyte Antigen Antibodies and Development of Antibody-Mediated Rejection. Transplantation (2011) 92(1):41–7. doi:10.1097/TP.0b013e31821cdf0d
114. Senev, A, Ray, B, Lerut, E, Hariharan, J, Heylen, C, Kuypers, D, et al. The Pre-transplant Non-HLA Antibody Burden Associates with the Development of Histology of Antibody-Mediated Rejection after Kidney Transplantation. Front Immunol (2022) 13:809059. doi:10.3389/fimmu.2022.809059
115. Wehmeier, C, Karahan, GE, Krop, J, de Vaal, Y, Langerak-Langerak, J, Binet, I, et al. Donor-specific B Cell Memory in Alloimmunized Kidney Transplant Recipients: First Clinical Application of a Novel Method. Transplantation (2020) 104(5):1026–32. doi:10.1097/TP.0000000000002909
116. Lucia, M, Luque, S, Crespo, E, Melilli, E, Cruzado, JM, Martorell, J, et al. Preformed Circulating HLA-specific Memory B Cells Predict High Risk of Humoral Rejection in Kidney Transplantation. Kidney Int (2015) 88(4):874–87. doi:10.1038/ki.2015.205
117. Visentin, J, Leu, DL, Mulder, A, Jambon, F, Badier, L, Lee, JH, et al. Measuring Anti-HLA Antibody Active Concentration and Affinity by Surface Plasmon Resonance: Comparison with the Luminex Single Antigen Flow Beads and T-Cell Flow Cytometry Crossmatch Results. Mol Immunol (2019) 108:34–44. doi:10.1016/j.molimm.2019.02.006
118. Senev, A, Lerut, E, Van Sandt, V, Coemans, M, Callemeyn, J, Sprangers, B, et al. Specificity, Strength, and Evolution of Pretransplant Donor-specific HLA Antibodies Determine Outcome after Kidney Transplantation. Am J Transpl (2019) 19(11):3100–13. doi:10.1111/ajt.15414
119. Marfo, K, Ajaimy, M, Colovai, A, Kayler, L, Greenstein, S, Lubetzky, M, et al. Pretransplant Immunologic Risk Assessment of Kidney Transplant Recipients with Donor-specific Anti-human Leukocyte Antigen Antibodies. Transplantation (2014) 98(10):1082–8. doi:10.1097/TP.0000000000000191
120. Redondo-Pachon, D, Perez-Saez, MJ, Mir, M, Gimeno, J, Llinas, L, Garcia, C, et al. Impact of Persistent and Cleared Preformed HLA DSA on Kidney Transplant Outcomes. Hum Immunol (2018) 79(6):424–31. doi:10.1016/j.humimm.2018.02.014
121. Caillard, S, Becmeur, C, Gautier-Vargas, G, Olagne, J, Muller, C, Cognard, N, et al. Pre-existing Donor-specific Antibodies Are Detrimental to Kidney Allograft Only when Persistent after Transplantation. Transpl Int (2017) 30(1):29–40. doi:10.1111/tri.12864
122. Susal, C, Wettstein, D, Dohler, B, Morath, C, Ruhenstroth, A, Scherer, S, et al. Association of Kidney Graft Loss with De Novo Produced Donor-specific and Non-donor-specific HLA Antibodies Detected by Single Antigen Testing. Transplantation (2015) 99(9):1976–80. doi:10.1097/TP.0000000000000672
123. Lefaucheur, C, Nochy, D, Hill, GS, Suberbielle-Boissel, C, Antoine, C, Charron, D, et al. Determinants of Poor Graft Outcome in Patients with Antibody-Mediated Acute Rejection. Am J Transpl (2007) 7(4):832–41. doi:10.1111/j.1600-6143.2006.01686.x
124. Adebiyi, OO, Gralla, J, Klem, P, Freed, B, Davis, S, Wiseman, AC, et al. Clinical Significance of Pretransplant Donor-specific Antibodies in the Setting of Negative Cell-Based Flow Cytometry Crossmatching in Kidney Transplant Recipients. Am J Transpl (2016) 16(12):3458–67. doi:10.1111/ajt.13848
125. Kimball, PM, Baker, MA, Wagner, MB, and King, A. Surveillance of Alloantibodies after Transplantation Identifies the Risk of Chronic Rejection. Kidney Int (2011) 79(10):1131–7. doi:10.1038/ki.2010.556
126. Higgins, R, Lowe, D, Hathaway, M, Lam, F, Kashi, H, Tan, LC, et al. Rises and Falls in Donor-specific and Third-Party HLA Antibody Levels after Antibody Incompatible Transplantation. Transplantation (2009) 87(6):882–8. doi:10.1097/TP.0b013e31819a6788
127. Burns, JM, Cornell, LD, Perry, DK, Pollinger, HS, Gloor, JM, Kremers, WK, et al. Alloantibody Levels and Acute Humoral Rejection Early after Positive Crossmatch Kidney Transplantation. Am J Transpl (2008) 8(12):2684–94. doi:10.1111/j.1600-6143.2008.02441.x
128. Phillpott, M, Daga, S, Higgins, R, Lowe, D, Krishnan, N, Zehnder, D, et al. Dynamic Behaviour of Donor Specific Antibodies in the Early Period Following HLA Incompatible Kidney Transplantation. Transpl Int (2022) 35:10128. doi:10.3389/ti.2022.10128
129. Reed, EF, Rao, P, Zhang, Z, Gebel, H, Bray, RA, Guleria, I, et al. Comprehensive Assessment and Standardization of Solid Phase Multiplex-Bead Arrays for the Detection of Antibodies to HLA-Drilling Down on Key Sources of Variation. Am J Transpl (2013) 13(11):3050–1. doi:10.1111/ajt.12462
130. Filippone, EJ, and Farber, JL. The Problem of Subclinical Antibody-Mediated Rejection in Kidney Transplantation. Transplantation (2021) 105(6):1176–87. doi:10.1097/TP.0000000000003543
131. Liu, W, Zhao, J, Kang, ZY, Xiao, YL, Yang, L, Liu, C, et al. De novo donor-specific HLA antibodies reduce graft survival rates and increase the risk of kidney transplant rejection: a single-center retrospective study. Transpl Immunol (2021) 68:101430.
132. Comoli, P, Cioni, M, Tagliamacco, A, Quartuccio, G, Innocente, A, Fontana, I, et al. Acquisition of C3d-Binding Activity by De Novo Donor-specific HLA Antibodies Correlates with Graft Loss in Nonsensitized Pediatric Kidney Recipients. Am J Transpl (2016) 16(7):2106–16. doi:10.1111/ajt.13700
133. Fylaktou, A, Karava, V, Vittoraki, A, Zampetoglou, A, Papachristou, M, Antoniadis, N, et al. Impact of De Novo Donor-specific HLA Antibodies on Pediatric Kidney Transplant Prognosis in Patients with Acute Declined or Stable Allograft Function. Pediatr Transpl (2022) 26(3):e14221. doi:10.1111/petr.14221
134. Heilman, RL, Nijim, A, Desmarteau, YM, Khamash, H, Pando, MJ, Smith, ML, et al. De Novo donor-specific Human Leukocyte Antigen Antibodies Early after Kidney Transplantation. Transplantation (2014) 98(12):1310–5. doi:10.1097/TP.0000000000000216
135. Kauke, T, Oberhauser, C, Lin, V, Coenen, M, Fischereder, M, Dick, A, et al. De Novo donor-specific Anti-HLA Antibodies after Kidney Transplantation Are Associated with Impaired Graft Outcome Independently of Their C1q-Binding Ability. Transpl Int (2017) 30(4):360–70. doi:10.1111/tri.12887
136. Lefaucheur, C, Loupy, A, Hill, GS, Andrade, J, Nochy, D, Antoine, C, et al. Preexisting Donor-specific HLA Antibodies Predict Outcome in Kidney Transplantation. J Am Soc Nephrol (2010) 21(8):1398–406. doi:10.1681/ASN.2009101065
137. Pernin, V, Beyze, A, Szwarc, I, Bec, N, Salsac, C, Perez-Garcia, E, et al. Distribution of De Novo Donor-specific Antibody Subclasses Quantified by Mass Spectrometry: High IgG3 Proportion Is Associated with Antibody-Mediated Rejection Occurrence and Severity. Front Immunol (2020) 11:919. doi:10.3389/fimmu.2020.00919
138. Freitas, MC, Rebellato, LM, Ozawa, M, Nguyen, A, Sasaki, N, Everly, M, et al. The Role of Immunoglobulin-G Subclasses and C1q in De Novo HLA-DQ Donor-specific Antibody Kidney Transplantation Outcomes. Transplantation (2013) 95(9):1113–9. doi:10.1097/TP.0b013e3182888db6
139. Viglietti, D, Loupy, A, Vernerey, D, Bentlejewski, C, Gosset, C, Aubert, O, et al. Value of Donor-specific Anti-HLA Antibody Monitoring and Characterization for Risk Stratification of Kidney Allograft Loss. J Am Soc Nephrol (2017) 28(2):702–15. doi:10.1681/ASN.2016030368
140. Neuberger, JM, Bechstein, WO, Kuypers, DR, Burra, P, Citterio, F, De Geest, S, et al. Practical Recommendations for Long-Term Management of Modifiable Risks in Kidney and Liver Transplant Recipients: A Guidance Report and Clinical Checklist by the Consensus on Managing Modifiable Risk in Transplantation (COMMIT) Group. Transplantation (2017) 101(2):S1–S56. doi:10.1097/TP.0000000000001651
141. Meziyerh, S, van Gelder, T, Kers, J, van der Helm, D, van der Boog, PJM, de Fijter, JW, et al. Tacrolimus and mycophenolic acid exposure are associated with biopsy-proven acute rejection: a study to provide evidence for longer-term target ranges. Clin Pharmacol Ther. (2023) Epub ahead of print.
142. Gold, A, Tonshoff, B, Dohler, B, and Susal, C Association of graft survival with tacrolimus exposure and late intra-patient tacrolimus variability in pediatric and young adult renal transplant recipients-an international CTS registry analysis. Transpl Int. (2020) 33(12):1681–92.
143. Brunet, M, van Gelder, T, Asberg, A, Haufroid, V, Hesselink, DA, Langman, L, et al. Therapeutic drug monitoring of tacrolimus-personalized therapy: second consensus report. Ther Drug Monit (2019) 41(3):261–307.
144. Susal, C, and Dohler, B Late intra-patient tacrolimus trough level variability as a major problem in kidney transplantation: a collaborative transplant study report. Am J Transplant (2019) 19(10):2805–13.
145. Sablik, KA, Clahsen-van Groningen, MC, Hesselink, DA, van Gelder, T, and Betjes, MGH. Tacrolimus intra-patient variability is not associated with chronic active antibody mediated rejection. PLoS One (2018) 13(5):e0196552.
146. Filler, G, Todorova, EK, Bax, K, Alvarez-Elias, AC, Huang, SH, and Kobrzynski, MC. Minimum mycophenolic acid levels are associated with donor-specific antibody formation. Pediatr Transplant (2016) 20(1):34–8.
147. Meziyerh, S, Bouwmans, P, van Gelder, T, van der Helm, D, Messchendorp, L, van der Boog, PJM, et al. Mycophenolic acid exposure determines antibody formation following SARS-CoV-2 vaccination in kidney transplant recipients: a nested cohort study. Clin Pharmacol Ther (2023).
148. Haller, MC, Royuela, A, Nagler, EV, Pascual, J, and Webster, AC. Steroid avoidance or withdrawal for kidney transplant recipients. Cochrane Database Syst Rev (2016) 2016(8):CD005632.
149. Mayer, KA, Doberer, K, Eskandary, F, Halloran, PF, and Bohmig, GA. New Concepts in Chronic Antibody-Mediated Kidney Allograft Rejection: Prevention and Treatment. Curr Opin Organ Transpl (2021) 26(1):97–105. doi:10.1097/MOT.0000000000000832
150. Jordan, SC, Ammerman, N, Choi, J, Huang, E, Peng, A, Sethi, S, et al. The Role of Novel Therapeutic Approaches for Prevention of Allosensitization and Antibody-Mediated Rejection. Am J Transpl (2020) 20(4):42–56. doi:10.1111/ajt.15913
151. Leibler, C, Matignon, M, Moktefi, A, Samson, C, Zarour, A, Malard, S, et al. Belatacept in Renal Transplant Recipient with Mild Immunologic Risk Factor: A Pilot Prospective Study (BELACOR). Am J Transpl (2019) 19(3):894–906. doi:10.1111/ajt.15229
152. Sethi, S, Najjar, R, Peng, A, Choi, J, Lim, K, Vo, A, et al. Outcomes of Conversion from Calcineurin Inhibitor to Belatacept-Based Immunosuppression in HLA-Sensitized Kidney Transplant Recipients. Transplantation (2020) 104(7):1500–7. doi:10.1097/TP.0000000000002976
153. Choi, M, Bachmann, F, Wu, K, Lachmann, N, Schmidt, D, Brakemeier, S, et al. Microvascular Inflammation Is a Risk Factor in Kidney Transplant Recipients with Very Late Conversion from Calcineurin Inhibitor-Based Regimens to Belatacept. BMC Nephrol (2020) 21(1):354. doi:10.1186/s12882-020-01992-6
154. Darres, A, Ulloa, C, Brakemeier, S, Garrouste, C, Bestard, O, Del Bello, A, et al. Conversion to Belatacept in Maintenance Kidney Transplant Patients: A Retrospective Multicenter European Study. Transplantation (2018) 102(9):1545–52. doi:10.1097/TP.0000000000002192
155. Everly, MJ, Terasaki, PI, and Trivedi, HL. Durability of Antibody Removal Following Proteasome Inhibitor-Based Therapy. Transplantation (2012) 93(6):572–7. doi:10.1097/TP.0b013e31824612df
156. Mehta, R, Sood, P, and Hariharan, S. Subclinical Rejection in Renal Transplantation: Reappraised. Transplantation (2016) 100(8):1610–8. doi:10.1097/TP.0000000000001163
157. Nankivell, BJ, Borrows, RJ, Fung, CL, O'Connell, PJ, Allen, RD, and Chapman, JR. Natural History, Risk Factors, and Impact of Subclinical Rejection in Kidney Transplantation. Transplantation (2004) 78(2):242–9. doi:10.1097/01.tp.0000128167.60172.cc
158. Moreso, F, Ibernon, M, Goma, M, Carrera, M, Fulladosa, X, Hueso, M, et al. Subclinical Rejection Associated with Chronic Allograft Nephropathy in Protocol Biopsies as a Risk Factor for Late Graft Loss. Am J Transpl (2006) 6(4):747–52. doi:10.1111/j.1600-6143.2005.01230.x
159. Scholten, EM, Rowshani, AT, Cremers, S, Bemelman, FJ, Eikmans, M, van Kan, E, et al. Untreated Rejection in 6-month Protocol Biopsies Is Not Associated with Fibrosis in Serial Biopsies or with Loss of Graft Function. J Am Soc Nephrol (2006) 17(9):2622–32. doi:10.1681/ASN.2006030227
160. Kurtkoti, J, Sakhuja, V, Sud, K, Minz, M, Nada, R, Kohli, HS, et al. The Utility of 1- and 3-month Protocol Biopsies on Renal Allograft Function: a Randomized Controlled Study. Am J Transpl (2008) 8(2):317–23. doi:10.1111/j.1600-6143.2007.02049.x
161. Rush, D, Nickerson, P, Gough, J, McKenna, R, Grimm, P, Cheang, M, et al. Beneficial Effects of Treatment of Early Subclinical Rejection: a Randomized Study. J Am Soc Nephrol (1998) 9(11):2129–34. doi:10.1681/ASN.V9112129
162. Choi, BS, Shin, MJ, Shin, SJ, Kim, YS, Choi, YJ, Kim, YS, et al. Clinical Significance of an Early Protocol Biopsy in Living-Donor Renal Transplantation: Ten-Year Experience at a Single center. Am J Transpl (2005) 5(6):1354–60. doi:10.1111/j.1600-6143.2005.00830.x
163. Seron, D, Rabant, M, Becker, JU, Roufosse, C, Bellini, MI, Bohmig, GA, et al. Proposed Definitions of T Cell-Mediated Rejection and Tubulointerstitial Inflammation as Clinical Trial Endpoints in Kidney Transplantation. Transpl Int (2022) 35:10135. doi:10.3389/ti.2022.10135
164. Rush, D, Arlen, D, Boucher, A, Busque, S, Cockfield, SM, Girardin, C, et al. Lack of Benefit of Early Protocol Biopsies in Renal Transplant Patients Receiving TAC and MMF: a Randomized Study. Am J Transpl (2007) 7(11):2538–45. doi:10.1111/j.1600-6143.2007.01979.x
165. Seifert, ME, Yanik, MV, Feig, DI, Hauptfeld-Dolejsek, V, Mroczek-Musulman, EC, Kelly, DR, et al. Subclinical Inflammation Phenotypes and Long-Term Outcomes after Pediatric Kidney Transplantation. Am J Transpl (2018) 18(9):2189–99. doi:10.1111/ajt.14933
166. Hoffman, W, Mehta, R, Jorgensen, DR, Sood, P, Randhawa, P, Wu, CM, et al. The Impact of Early Clinical and Subclinical T Cell-Mediated Rejection after Kidney Transplantation. Transplantation (2019) 103(7):1457–67. doi:10.1097/TP.0000000000002560
167. Ho, J, Okoli, GN, Rabbani, R, Lam, OLT, Reddy, VK, Askin, N, et al. Effectiveness of T Cell-Mediated Rejection Therapy: A Systematic Review and Meta-Analysis. Am J Transpl (2022) 22(3):772–85. doi:10.1111/ajt.16907
168. Leblanc, J, Subrt, P, Pare, M, Hartell, D, Senecal, L, Blydt-Hansen, T, et al. Practice Patterns in the Treatment and Monitoring of Acute T Cell-Mediated Kidney Graft Rejection in Canada. Can J Kidney Health Dis (2018) 5:2054358117753616. doi:10.1177/2054358117753616
169. Sood, P, Cherikh, WS, Toll, AE, Mehta, RB, and Hariharan, S. Kidney Allograft Rejection: Diagnosis and Treatment Practices in USA- A UNOS Survey. Clin Transpl (2021) 35(4):e14225. doi:10.1111/ctr.14225
170. Lachmann, N, Duerr, M, Schonemann, C, Pruss, A, Budde, K, and Waiser, J. Treatment of Antibody-Mediated Renal Allograft Rejection: Improving Step by Step. J Immunol Res (2017) 2017:6872046. doi:10.1155/2017/6872046
171. Eskandary, F, Durr, M, Budde, K, Doberer, K, Reindl-Schwaighofer, R, Waiser, J, et al. Clazakizumab in Late Antibody-Mediated Rejection: Study Protocol of a Randomized Controlled Pilot Trial. Trials (2019) 20(1):37. doi:10.1186/s13063-018-3158-6
172. Doberer, K, Duerr, M, Halloran, PF, Eskandary, F, Budde, K, Regele, H, et al. A Randomized Clinical Trial of Anti-IL-6 Antibody Clazakizumab in Late Antibody-Mediated Kidney Transplant Rejection. J Am Soc Nephrol (2021) 32(3):708–22. doi:10.1681/ASN.2020071106
173. Mayer, KA, Budde, K, Halloran, PF, Doberer, K, Rostaing, L, Eskandary, F, et al. Safety, Tolerability, and Efficacy of Monoclonal CD38 Antibody Felzartamab in Late Antibody-Mediated Renal Allograft Rejection: Study Protocol for a Phase 2 Trial. Trials (2022) 23(1):270. doi:10.1186/s13063-022-06198-9
174. Roufosse, C, Becker, JU, Rabant, M, Seron, D, Bellini, MI, Bohmig, GA, et al. Proposed Definitions of Antibody-Mediated Rejection for Use as a Clinical Trial Endpoint in Kidney Transplantation. Transpl Int (2022) 35:10140. doi:10.3389/ti.2022.10140
175. Orandi, BJ, Chow, EH, Hsu, A, Gupta, N, Van Arendonk, KJ, Garonzik-Wang, JM, et al. Quantifying Renal Allograft Loss Following Early Antibody-Mediated Rejection. Am J Transpl (2015) 15(2):489–98. doi:10.1111/ajt.12982
176. Mohnen, SM, van Oosten, MJM, Los, J, Leegte, MJH, Jager, KJ, Hemmelder, MH, et al. Healthcare Costs of Patients on Different Renal Replacement Modalities - Analysis of Dutch Health Insurance Claims Data. PLoS One (2019) 14(8):e0220800. doi:10.1371/journal.pone.0220800
177. Kiberd, BA, Miller, A, Martin, S, and Tennankore, KK. De Novo Donor-Specific Human Leukocyte Antigen Antibody Screening in Kidney Transplant Recipients after the First Year Posttransplantation: A Medical Decision Analysis. Am J Transpl (2016) 16(11):3212–9. doi:10.1111/ajt.13838
178. Lachmann, N, Niemann, M, Reinke, P, Budde, K, Schmidt, D, Halleck, F, et al. Donor-Recipient Matching Based on Predicted Indirectly Recognizable HLA Epitopes Independently Predicts the Incidence of De Novo Donor-specific HLA Antibodies Following Renal Transplantation. Am J Transpl (2017) 17(12):3076–86. doi:10.1111/ajt.14393
179. Ginevri, F, Nocera, A, Comoli, P, Innocente, A, Cioni, M, Parodi, A, et al. Posttransplant De Novo Donor-specific Hla Antibodies Identify Pediatric Kidney Recipients at Risk for Late Antibody-Mediated Rejection. Am J Transpl (2012) 12(12):3355–62. doi:10.1111/j.1600-6143.2012.04251.x
180. Lachmann, N, Terasaki, PI, Budde, K, Liefeldt, L, Kahl, A, Reinke, P, et al. Anti-human Leukocyte Antigen and Donor-specific Antibodies Detected by Luminex Posttransplant Serve as Biomarkers for Chronic Rejection of Renal Allografts. Transplantation (2009) 87(10):1505–13. doi:10.1097/TP.0b013e3181a44206
181. Liefeldt, L, Brakemeier, S, Glander, P, Waiser, J, Lachmann, N, Schonemann, C, et al. Donor-specific HLA Antibodies in a Cohort Comparing Everolimus with Cyclosporine after Kidney Transplantation. Am J Transpl (2012) 12(5):1192–8. doi:10.1111/j.1600-6143.2011.03961.x
182. Devos, JM, Gaber, AO, Teeter, LD, Graviss, EA, Patel, SJ, Land, GA, et al. Intermediate-term Graft Loss after Renal Transplantation Is Associated with Both Donor-specific Antibody and Acute Rejection. Transplantation (2014) 97(5):534–40. doi:10.1097/01.TP.0000438196.30790.66
183. Everly, MJ, Rebellato, LM, Haisch, CE, Ozawa, M, Parker, K, Briley, KP, et al. Incidence and Impact of De Novo Donor-specific Alloantibody in Primary Renal Allografts. Transplantation (2013) 95(3):410–7. doi:10.1097/TP.0b013e31827d62e3
184. Loucks-DeVos, JM, Eagar, TN, Gaber, AO, Patel, SJ, Teeter, LD, Graviss, EA, et al. The Detrimental Impact of Persistent vs an Isolated Occurrence of De Novo Donor-specific Antibodies on Intermediate-Term Renal Transplant Outcomes. Clin Transplant (2017) 31(8):e13025. doi:10.1111/ctr.13025
185. Cross, AR, Lion, J, Poussin, K, Assayag, M, Taupin, JL, Glotz, D, et al. HLA-DQ Alloantibodies Directly Activate the Endothelium and Compromise Differentiation of FoxP3(high) Regulatory T Lymphocytes. Kidney Int (2019) 96(3):689–98. doi:10.1016/j.kint.2019.04.023
186. Lachmann, N, Niemann, M, Reinke, P, Budde, K, Schmidt, D, Halleck, F, et al. Donor-Recipient Matching Based on Predicted Indirectly Recognizable HLA Epitopes Independently Predicts the Incidence of De Novo Donor-specific HLA Antibodies Following Renal Transplantation. Am J Transplant (2017) 17(12):3076–86. doi:10.1111/ajt.14393
187. Bestard, O, Meneghini, M, Crespo, E, Bemelman, F, Koch, M, Volk, HD, et al. Preformed T Cell Alloimmunity and HLA Eplet Mismatch to Guide Immunosuppression Minimization with Tacrolimus Monotherapy in Kidney Transplantation: Results of the CELLIMIN Trial. Am J Transpl (2021) 21(8):2833–45. doi:10.1111/ajt.16563
Keywords: DSA, donor-specific HLA antibodies, biomarker, guidelines, subclinical rejection, monitoring
Citation: van den Broek DAJ, Meziyerh S, Budde K, Lefaucheur C, Cozzi E, Bertrand D, López del Moral C, Dorling A, Emonds M-P, Naesens M, de Vries APJ and the ESOT Working Group Subclinical DSA Monitoring (2023) The Clinical Utility of Post-Transplant Monitoring of Donor-Specific Antibodies in Stable Renal Transplant Recipients: A Consensus Report With Guideline Statements for Clinical Practice. Transpl Int 36:11321. doi: 10.3389/ti.2023.11321
Received: 01 March 2023; Accepted: 22 June 2023;
Published: 25 July 2023.
Copyright © 2023 van den Broek, Meziyerh, Budde, Lefaucheur, Cozzi, Bertrand, López del Moral, Dorling, Emonds, Naesens, de Vries and the ESOT Working Group Subclinical DSA Monitoring. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dennis A. J. van den Broek, ZC5hLmoudmFuX2Rlbl9icm9la0BsdW1jLm5s
†ORCID: Dennis A. J. van den Broek, orcid.org/0000-0001-7135-4752; Soufian Meziyerh, orcid.org/0000-0001-7694-8381; Klemens Budde, orcid.org/0000-0002-7929-5942; Carmen Lefaucheur, orcid.org/0000-0002-6244-0795; Emanuele Cozzi, orcid.org/0000-0001-7855-5055; Covadonga López del Moral, orcid.org/0000-0002-0613-2595; Anthony Dorling, orcid.org/0000-0003-3102-2600; Marie-Paule Emonds, orcid.org/0000-0002-2653-8656; Maarten Naesens, orcid.org/0000-0002-5625-0792; Aiko P. J. de Vries, orcid.org/0000-0002-9284-3595