 Lorenzo Piemonti1*
Lorenzo Piemonti1* Hanne Scholz2
Hanne Scholz2 Dide de Jongh3,4
Dide de Jongh3,4 Julie Kerr-Conte5
Julie Kerr-Conte5 Aart van Apeldoorn6
Aart van Apeldoorn6 James A. M. Shaw7Marten A. Engelse8
James A. M. Shaw7Marten A. Engelse8 Eline Bunnik3Markus Mühlemann9Karolina Pal-Kutas9William E. Scott III7Jérémy Magalon10,11Patrick Kugelmeier9†
Eline Bunnik3Markus Mühlemann9Karolina Pal-Kutas9William E. Scott III7Jérémy Magalon10,11Patrick Kugelmeier9† Ekaterine Berishvili12†
Ekaterine Berishvili12†- 1Diabetes Research Institute, IRCCS Ospedale San Raffaele and Vita-Salute San Raffaele University, Milan, Italy
- 2Department of Transplant Medicine and Institute for Surgical Research, Oslo University Hospital, Oslo, Norway
- 3Department of Medical Ethics, Philosophy and History of Medicine, Erasmus MC, University Medical Centre Rotterdam, Rotterdam, Netherlands
- 4Department of Nephrology and Transplantation, Erasmus MC, University Medical Centre Rotterdam, Rotterdam, Netherlands
- 5Université de Lille, INSERM, Campus Hospitalo-Universitaire de Lille, Institut Pasteur de Lille, U1190-EGID, Lille, France
- 6Department CBITE, MERLN Institute for Technology-Inspired Regenerative Medicine, Maastricht University, Maastricht, Netherlands
- 7Translational and Clinical Research Institute, The Medical School, Newcastle University, Newcastle upon Tyne, United Kingdom
- 8Nephrology, Leiden University Medical Center, Leiden, Netherlands
- 9Kugelmeiers Ltd., Zollikerberg, Switzerland
- 10Laboratoire de Culture et Thérapie Cellulaire, Assistance Publique des Hôpitaux de Marseille, Marseille, France
- 11Vascular Research Center Marseille, INSERM UMRS 1076, Faculté de Pharmacie, Marseille, France
- 12Laboratory of Tissue Engineering and Organ Regeneration, Department of Surgery, University of Geneva, Geneva, Switzerland
The field of transplantation has witnessed the emergence of Advanced Therapy Medicinal Products (ATMPs) as highly promising solutions to address the challenges associated with organ and tissue transplantation. ATMPs encompass gene therapy, cell therapy, and tissue-engineered products, hold immense potential for breakthroughs in overcoming the obstacles of rejection and the limited availability of donor organs. However, the development and academic research access to ATMPs face significant bottlenecks that hinder progress. This opinion paper emphasizes the importance of addressing bottlenecks in the development and academic research access to ATMPs by implementing several key strategies. These include the establishment of streamlined regulatory processes, securing increased funding for ATMP research, fostering collaborations and partnerships, setting up centralized ATMP facilities, and actively engaging with patient groups. Advocacy at the policy level is essential to provide support for the development and accessibility of ATMPs, thereby driving advancements in transplantation and enhancing patient outcomes. By adopting these strategies, the field of transplantation can pave the way for the introduction of innovative and efficacious ATMP therapies, while simultaneously fostering a nurturing environment for academic research.
Advanced Therapy Medicinal Products (ATMPs) defined in Regulation (EC) No 1394/2007 in the European Union, are medicinal products for human use including gene therapy medicinal products (GTMP), somatic cell therapy medicinal products (sCTMP), tissue-engineered products (TEP), or combinations of these [1]. The European Medicines Agency (EMA) regulates ATMPs through the Committee for Advanced Therapies (CAT), which provides scientific advice and evaluates marketing authorization applications for ATMPs based on quality, safety, and efficacy. The CAT’s opinion forms the basis for marketing authorization by the European Commission. As of the most recent published report (Figure 1, quarterly highlights and approved ATMPs, 2009-January 2023), the CAT provided 597 scientific recommendations on ATMPs, 559 scientific advice to companies, and reviewed 116 applications for Priority Medicines designation, granting 50 of them. The first ATMP to receive authorization in the EU was ChondroCelect®, a tissue-engineered product used for treating cartilage defects in 2009, followed by Glybera®, the first gene therapy, in 2012, and PROVENGE®, the first somatic cell therapy, in 2013.
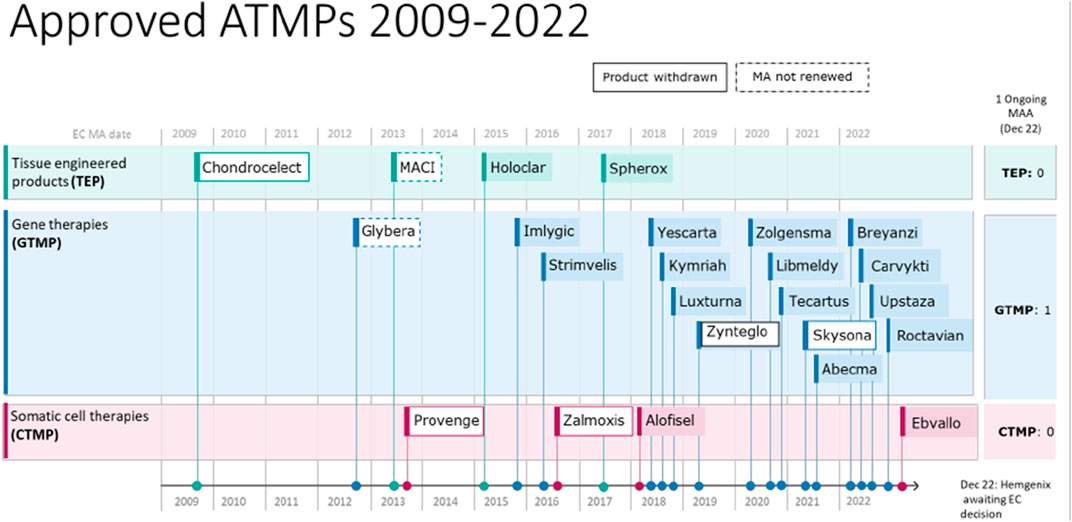
FIGURE 1. Summary of authorized Advanced Therapy Medicinal Products (ATMPs) between 2009 and 2022, encompassing both withdrawn or non-renewed ones. Source: [2].
The field of ATMPs is still relatively new, and the number of Marketing Authorization Applications (MAAs) submitted to CAT remains low [3]. Despite the high level of presubmission activity, the CAT only received 36 MAAs for ATMPs and authorized 25 of them (Table 1). This is partly due to the complex and challenging nature of developing ATMPs, which often requires a significant investment of time and resources to achieve regulatory approval [4, 5]. One reason for the slow take/emergence of ATMPs is the limited patient populations for rare diseases, which makes it challenging to conduct clinical trials and demonstrate safety and efficacy [6]. Another factor is the evolving regulatory landscape, which requires the establishment of clear guidelines and standards for the development and approval of these therapies. Additionally, ATMPs are often developed for diseases with limited treatment options, which can pose additional challenges for clinical trial design and regulatory approval (i.e., small patient populations, disease heterogeneity, lack of established endpoints, limited comparative data, long-term follow-up requirements, regulatory complexities, and specialized manufacturing).
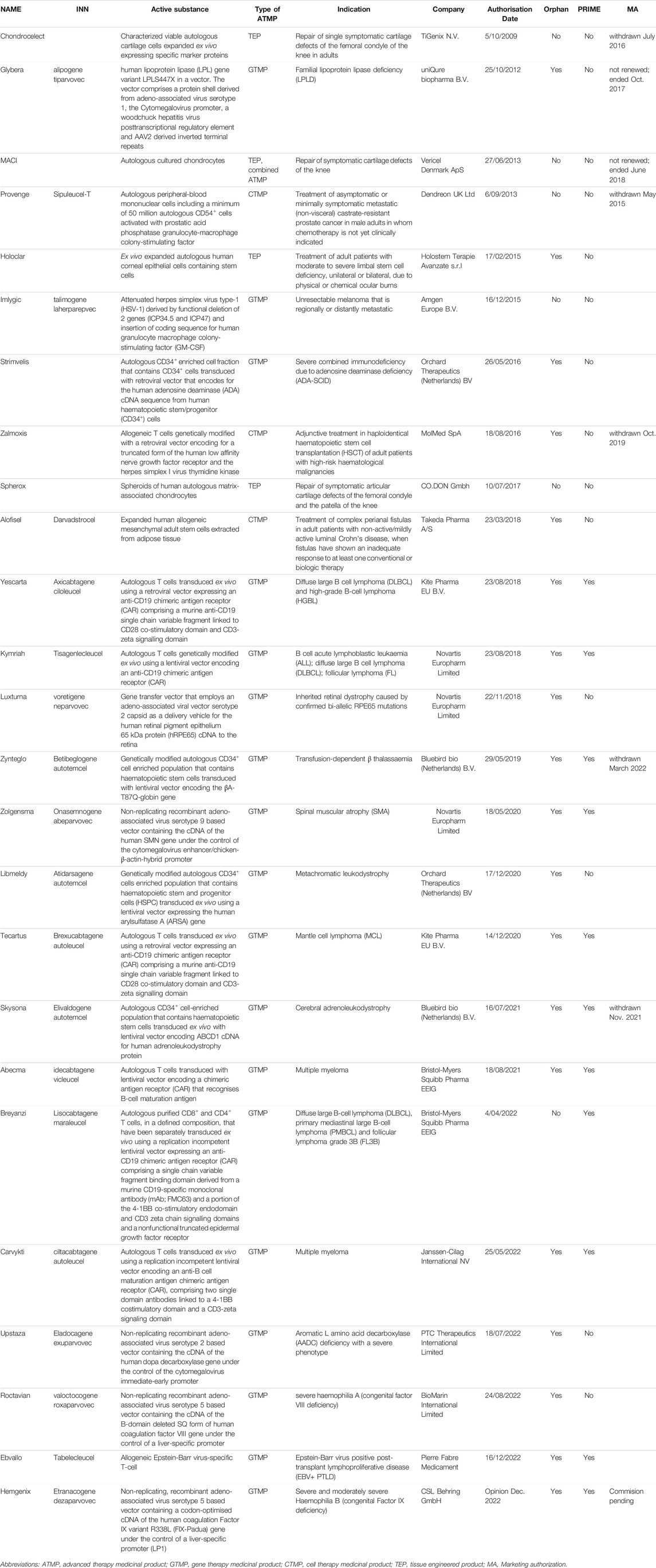
TABLE 1. List of authorised ATMPs by EMA.
Regarding the authorization of MAAs, it is worth noting that the CAT in the European Union maintains stringent requirements for evidence of quality, safety, and efficacy before granting marketing authorization for ATMPs [7]. This rigorous approval process implies that not all MAAs submitted will be authorized, and certain products may necessitate additional data or further development to meet the necessary criteria. Furthermore, continuous monitoring and surveillance of authorized ATMPs are conducted, and the CAT may request supplementary data or undertake regulatory measures if concerns arise regarding safety or efficacy. This ongoing monitoring ensures that ATMPs continue to meet the required standards of quality, safety, and efficacy after being authorized for marketing. European Union has implemented various measures to tackle the challenges associated with the approval of ATMPs. One such measure involves the establishment of incentives to support the development of orphan drugs, including ATMPs. Orphan drugs are specifically designed to treat rare diseases that affect a relative small number of patients. Companies engaged in the development of orphan drugs, including ATMPs, can be encouraged by several incentives, such as market exclusivity, reduced fees, protocol assistance, and eligibility for EU research funding. Additionally, the EU has introduced a regulatory pathway known as “conditional marketing authorization.” This pathway enables expedited access to medicines that address unmet medical needs. Conditional approval can be granted to ATMPs and other drugs based on promising initial data. This regulation assures that the medicine meets strict EU standards for safety, quality and efficacy, and that suppporting data is still generated post-approval to complete its safety profile. The most recent example which allowed fast track authorization is the COVID-19 vaccines which were released in the EU to support the mass vaccination campaign against the corona virus. Companies that receive conditional approval are required to provide further evidence to substantiate the benefits of the medicine, thus allowing patients to access potentially life-saving treatments at an earlier stage. These measures are aimed at promoting the development of ATMPs and improving access to innovative therapies for patients affected by rare diseases or unmet medical needs. However, despite these encouragments, they may not be sufficiently effective to facilitate widespread approval and dissemination of ATMPs.
The sluggish approval process for ATMPs has various implications that warrant concern [8]. Foremost among these is the potential to leave patients with rare and complex diseases without access to life-saving treatments [9]. The delay in approvals can prolong their suffering and even lead to unnecessary fatalities, while the social economic effects of their disease lead to increased healthcare costs and less access to the labor market. Furthermore, the restricted adoption of ATMPs may impede scientific advancement in regenerative medicine and cell therapy, as they offer a new and promising means of treating diseases, as more positive examples could lead to increased interest from the scientific community to explore these alternatives. A limited number of approved ATMPs could discourage investors and researchers from pursuing this area of research, leading to a lack of progress in creating innovative cell therapies. Moreover, the high costs associated with developing ATMPs may cause companies to be wary of investing in them without a comprehensive understanding of regulatory requirements and commercial viability. The tardiness in approvals could intensify this hesitancy, leading to a decline in investment in ATMPs and a deceleration in the development of new treatments.
The challenges that ATMPs face in overcoming the “economic valley of death” after obtaining marketing authorization have raised even greater concerns [10]. In fact, out of the 25 authorized ATMPs, seven had their marketing authorization withdrawn or not renewed. It is evident that the financial commitment for earlier trials, even in academic settings, is considerably high and the cost of upgrading an ATMP manufacturing process to obtain GMP certification is substantial, often exceeding that of similar clinical-grade cell products by 2–3 times. To make the process economically sustainable, academic scientists have established collaborations with small or large companies or founded biotechnology start-ups [11]. Nonetheless, the investments needed to take an ATMP to marketing authorization are very high, not only due to the costs of running clinical trials, but also the manufacturing costs of viral vectors and cellular products, as well as the stringent standards imposed by regulatory agencies to ensure the safety and quality of these products. Furthermore, the patient population that would benefit from these therapies is often very small, ranging from several thousand for less rare diseases to a few dozen for very rare diseases. The high costs of research and development and production have resulted in companies demanding very high prices for these therapies, ranging from several hundred thousand to a few million euros per patient. This can cause lengthy negotiations or even rejection by National Health Systems unwilling to cover the costs, even for a few patients. As a result, some efficacious and approved products, such as Skysona for adrenoleukodystrophy and Zynteglo for beta-thalassemia, have been withdrawn from the European market, leaving patients who might have benefited from these life-saving therapies without access to them. Secondly, companies may decide to drop an approved ATMP, even when it is approved and when a reimbursement policy has been negotiated, simply due to insufficient economic return [12]. This is particularly true for rare diseases where the very low number of patients poses significant challenges. For instance, Glybera, an approved gene therapy product for Type I hyperlipoproteinemia, withdrew after treating only one patient. Similarly, Strimvelis®, the first ex vivo gene therapy product approved in Europe, was passed on to Orchard Therapeutics after being created by GSK and the San Raffaele Telethon Institute of Gene Therapy in Milan. While the therapy proved effective in treating some patients, Orchard Therapeutics recently pulled it from the market due to commercial considerations. Finally, Valline Holding Srl made the decision to cease financial backing to Holostem, the company responsible for creating Holoclar®, the first stem cell-derived ATMP approved in Europe.
Developing ATMPs for rare diseases is crucial to the advancement of medical innovation and technology transfer [13]. The development of these therapies requires significant investments in research, development, infrastructure, and regulatory frameworks, which can be leveraged to develop treatments for more common diseases. This approach encourages collaborations between academic institutions, industry partners, and regulatory agencies, stimulating innovation and accelerating the translation of research into clinical applications. In addition, the development of ATMPs for rare diseases can create an ecosystem that supports innovation and technology transfer. Researchers and developers can use these rare diseases as a platform to refine cutting-edge technologies, such as gene editing and stem cell therapies, which can then be applied to other disease areas with similar genetic and cellular foundations, such as cancer or neurodegenerative diseases. Moreover, developing ATMPs for rare diseases can spur investment in related fields, including manufacturing and supply chain logistics, helping to lower the production costs and improve the scalability of ATMPs, ultimately making them more accessible to patients worldwide.
ATMPs are extremely relevant to the field of transplantation as they offer a promising way to address many of the challenges associated with organ and tissue transplantation [14, 15]. One of the main challenges of transplantation is rejection, which occurs when the recipient’s immune system recognizes the transplanted organ or tissue as foreign and attacks it. Immunosuppressive therapy is currently used to prevent rejection, but this can have significant side effects and long-term complications, including increased susceptibility to infections and cancer. ATMPs offer a potential solution to this problem by modifying the recipient’s immune system to accept the transplanted organ or tissue as “self.” For example, chimeric antigen receptor (CAR) T cell therapy involves genetically engineering the patient’s own immune cells to target and destroy cancer cells [16]. This approach has shown promise in treating post-transplant lymphoproliferative disorders, which are a common complication of solid organ transplantation. Another ATMP approach is the use of regulatory T cells (Tregs), which are a subset of immune cells that play a key role in immune tolerance [17]. Treg therapy is being developed to induce immune tolerance and reduce the need for immunosuppressive therapy, which could improve patient outcomes and reduce the risk of complications. ATMPs are also being used to address other challenges associated with transplantation, such as the limited availability of donor organs and tissues. Tissue engineering is one approach that involves using biodegradable scaffolds and cells to create functional replacements for damaged or diseased tissues (cartilage, bone, skin, vessels, islet, etc.). Xenotransplantation is another approach that involves transplanting organs or tissues from one species to another. ATMPs such as gene editing and immune cell therapies are being developed to overcome the immunological barriers associated with xenotransplantation and make it a viable option for treating organ failure.
The field of transplantation is at a critical juncture, as there is an urgent need to address the challenges associated with organ and tissue transplantation. ATMPs offer a promising way to achieve this goal, but their development and access to academic research must be sustained and expanded to fully realize their potential [18]. The transplant community has a critical role to play in sustaining the ATMP field, as they are uniquely positioned to identify the unmet needs and opportunities for innovation in transplantation. This includes advocating for increased funding for ATMP research and development, as well as promoting collaborations between academic researchers, industry partners, and regulatory agencies to accelerate the translation of promising ATMP therapies to the clinic. In addition, the transplant community can support the development and adoption of innovative approaches to transplant surgery, such as ex vivo organ perfusion, which has been shown to improve the quality of donor organs and increase the number of viable organs available for transplantation. By embracing new technologies and approaches to transplantation, the transplant community can create a more supportive environment for the development and adoption of ATMPs. Moreover, it is essential that the transplant community engage in ongoing education and training on the latest advances in ATMPs, including their potential clinical applications, regulatory considerations, and ethical implications. This will ensure that transplant clinicians and researchers are equipped with the knowledge and skills needed to effectively translate and apply ATMPs in the clinical setting. Ultimately, the success of the ATMP field in transplantation will depend on the sustained commitment and collaboration of the transplant community. By working together to overcome the regulatory and funding challenges associated with ATMP development and access, the transplant community can help to ensure that patients in need of organ and tissue transplantation have access to the most innovative and effective therapies available. The timely and invaluable action of launching a task force by the European Society of Organ Transplantation (ESOT) to address ATM field issues in Europe demonstrates a recognition of the pressing challenges faced in the academic institution. It highlights a strong commitment to finding effective solutions. By assembling experts and stakeholders, the task force can capitalize on their collective knowledge and expertise to address crucial issues, fostering innovation, efficiency, and safety in European member states.
More specifically, to overcome the bottleneck in the development and access to ATMPs for academic research in the field of transplantation, several strategies can be implemented [19, 20]:
i) Streamlining regulatory processes. One of the major barriers to the development and access of ATMPs is the complex and lengthy regulatory approval process. To overcome this bottleneck, regulatory agencies can work to streamline their processes and reduce the time and cost of approval, while still ensuring the safety and efficacy of these therapies [21]. The EMA/CAT definition of ATMPS warrants reconsideration. Is it appropriate to regulate minimally modified cell therapy products, such as Stromal Vascular Fraction (SVF) differently based on non-homologous (ATMP) versus homologous therapy (simple cell therapy)? For instance, comparing SVF for plastic surgery (simple cell therapy) and SVF for scleroderma (ATMP), should not the classification be determined by the manufacturing process rather than the clinical end use? Could production facilities conduct risk assessments as evidence of manufacturing process quality?
ii) Increasing funding for ATMP research. The development of ATMPs requires significant investment in research and development. A challenge arises from the fact that public funding typically does not support these endeavors. National science funding primarily prioritizes the creation of new knowledge, focusing on academic research rather than the establishment of clinical trials or conducting safety studies, activities classified as TRL4 and higher in the EU. Consequently, scaling up an ATMP becomes unfeasible due to insufficient funding. To support this, funding agencies can increase their investment in ATMP research, with a focus on academic research and development.
iii) Promoting collaborations and partnerships. Collaboration between academic researchers, industry partners, and regulatory agencies is critical to the development and translation of ATMPs. To facilitate this, there is a need for increased support for partnerships and collaborations, including funding, infrastructure, and regulatory support.
iv) Establishing/Supporting Pre-ATMP Facilities. The development of pre-ATMP facilities is crucial for improving the efficiency and success rate of ATMP projects. It provides researchers with a valuable platform to thoroughly test their products, ensuring compatibility, safety, and efficacy before committing significant resources to full-scale GMP production. By avoiding potential pitfalls related to raw material and starting material selection early on, researchers can streamline the translation of ATMPs into clinical trials, fostering a more effective and efficient development pathway.
v) Establishing centralized ATMP facilities. The successful development and production of ATMPs rely on specialized facilities and expertise. To address the limited availability of these resources, the establishment of centralized ATMP facilities can provide academic researchers with accessible infrastructure and regulatory affairs expertise. This point is crucial, as it emphasizes the importance of not only having such facilities but also ensuring their affordability and having the necessary regulatory affairs expertise readily available. Having a cleanroom facility alone is insufficient for achieving clinical translation. The progress towards this goal can greatly benefit from experts who possess knowledge not only about regulatory hurdles but also about establishing effective quality management systems, training personnel in Good Manufacturing Practices (GMP), defining release criteria, and navigating other approval requirements. Typically, one option is to rent a cleanroom facility and seek the assistance of consultants for regulatory affairs. Additionally, safety studies are often outsourced to third-party organizations with ISO certification. However, this approach tends to be expensive, and obtaining research funding for these activities can be extremely challenging. This is because they extend beyond the scope of academic work and require substantial financial investments. Consequently, a gap is created presenting significant obstacles in terms of both financial resources and expertise for research groups interested in pursuing ATMP development. It would be beneficial if centralized facilities could offer a cost-effective combination of services specifically designed for academic researchers.
vi) Enhancing the efficiency and accessibility of the “Hospital Exemption” (HE) approval pathway. The HE pathway, a regulatory framework outlined in European Regulation No 1394/2007, provides a means for manufacturing and utilizing ATMPs outside the standard centralized marketing authorization pathway, subject to specific conditions. In February 2021, ARI-0001 (CART19-BE-01), an ATMP designed to target CD19+ B-cell malignancies, achieved a significant milestone [22]. The Spanish Agency of Medicines and Medical Devices (AEMPS) authorized its use under the HE pathway for treating adult patients over 25 years old with relapsed/refractory acute lymphoblastic leukemia. This achievement is remarkable as ARI-0001 becomes the first CAR-T therapy to receive approval from a governmental drug agency outside the central marketing authorization pathway. However, it is important to acknowledge the emergence of divergent interpretations and variations in HE implementation across countries and within industrial or academic organizations. These differences [8, 23–26] underline the need for greater harmonization of HE rules. While it is widely agreed that the HE pathway should not be exploited to bypass established procedures for marketing authorization and clinical trials in Europe, different viewpoints exist regarding the reasons for utilizing this pathway. Academic organizations emphasize the need to ensure uninterrupted patient treatment during clinical development, reduce costs, provide therapeutic options for individuals ineligible for clinical studies, accommodate early stages of product development with rapid manufacturing and advancements, and enable access to ATMPs with limited commercial viability that may not progress towards marketing authorization. Conversely, industrial organizations primarily raise concerns about the potential risks associated with establishing a dual-tier system with varying regulatory standards. Numerous challenges are associated with the HE pathway that necessitate attention: a) the lack of harmonization of HE rules among EU Member States, b) the necessity to enhance flexibility and efficiency in the regulatory process for HE-ATMPs, where even minor product modifications are regarded as “new products,” c) the substantial requirement of human, logistic, and financial resources, which pose barriers for both public facilities and private investors, particularly small and medium enterprises, d) ensuring access to HE-ATMPs for patients treated in hospitals other than the one involved in product development, and e) facilitating technology transfer and knowledge sharing to promote access to these therapies in hospitals within or beyond the Member State.
vii) Engaging with patients and patient advocacy groups. Patients and patient advocacy groups should have an important role in the clinical development and translational process of ATMPs. Early exploration and engagement of patient perspectives are essential to understand and address the barriers and facilitating factors that may affect the uptake and impact of ATMPS on patient communities. Empirical research on patient perspectives is therefore important in order to ensure responsible clinical translation of ATMPs.
Finally, accessibility implies not only availability, but also affordability [27]. Given the expected high prices of ATMPs, there are concerns about equitable distribution of ATMPs. However, especially in countries in which ATMP facilities and trained staff are lacking, these treatments may not become accessible to patients who may need them most. To provide equitable access to ATMPs across different regions and communities, investments must be made in robust supply chains and knowledge sharing. Even in less resource-constrained settings, strategies for fair pricing will be required, as well as adequate reimbursement policies and the provision of support programs to alleviate financial burdens on individual patients. Particular attention should be paid to individuals with rare diseases, as they often face significant challenges in accessing effective treatments. Achieving fair distribution of ATMPs entails addressing patients’ needs, including by raising awareness, improving early diagnosis, and establishing support networks. By doing so, we can ensure that patients with unmet medical needs have equitable opportunities to benefit from ATMPs. Equity in ATMPs extends to the realm of clinical trials as well. It is essential to ensure the inclusion of diverse populations, including historically underrepresented groups, in research studies. This inclusive approach enables a comprehensive understanding of the benefits and risks of ATMPs across various patient populations, thereby avoiding potential biases and ensuring equitable access to the benefits of research. Lastly, global disparities must be addressed to achieve equity in access to ATMPs. Efforts should be made to bridge gaps between different countries and regions, allowing individuals worldwide to benefit from these therapies. This can be accomplished through international collaboration, regulatory harmonization, and the transfer of knowledge and technology. By placing fair distribution of ATMPs at the center of our ethical considerations, we can work collectively to establish a healthcare landscape where all individuals, regardless of their socio-economic status, disease rarity, geographic location, or background, have equitable access to the transformative potential of ATMPs.
To claim for a new time, it is important to advocate for changes at the policy level that support the development and access to ATMPs for academic research [28]. This includes advocating for increased funding, streamlined regulatory processes, engagement of patients and patients advocacies and collaboration between academic researchers, industry partners, and regulatory agencies [29]. By working together to overcome the bottleneck in the development and access of ATMPs, we can create a more supportive environment for innovation in the field of transplantation and help to improve patient outcomes.
Data Availability Statement
Publicly available datasets were analyzed in this study. This data can be found here: [2].
Author Contributions
LP, PK, and EB contributed to conception and design of the study. LP wrote the first draft of the manuscript. HS, DJ, JK-C, and AA wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
Authors MM, KP-K, and PK were employed by Kugelmeiers Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Iglesias-Lopez, C, Obach, M, Vallano, A, and Agustí, A. Comparison of Regulatory Pathways for the Approval of Advanced Therapies in the European Union and the United States. Cytotherapy (2021) 23(3):261–74. doi:10.1016/j.jcyt.2020.11.008
2. European Medicines Agency. CAT Quarterly Highlights and Approved ATMPs - January 2023 (2023). Available from: https://www.ema.europa.eu/en/documents/report/cat-quarterly-highlights-approved-atmps-january-2023_en.pdf (Accessed September 22, 2023).
3. Coppens, D, De Wilde, S, Guchelaar, H, De Bruin, M, Leufkens, H, Meij, P, et al. A Decade of Marketing Approval of Gene and Cell-Based Therapies in the United States, European Union and Japan: An Evaluation of Regulatory Decision-Making. Cytotherapy (2018) 20(6):769–78. doi:10.1016/j.jcyt.2018.03.038
4. Shukla, V, Seoane-Vazquez, E, Fawaz, S, Brown, L, and Rodriguez-Monguio, R. The Landscape of Cellular and Gene Therapy Products: Authorization, Discontinuations, and Cost. Hum Gene Ther Clin Dev (2019) 30(3):102–13. doi:10.1089/humc.2018.201
5. Ten Ham, RM, Hoekman, J, Hövels, AM, Broekmans, AW, Leufkens, HG, and Klungel, OH. Challenges in Advanced Therapy Medicinal Product Development: A Survey Among Companies in Europe. Mol Therapy-Methods Clin Dev (2018) 11:121–30. doi:10.1016/j.omtm.2018.10.003
6. Aiuti, A, Pasinelli, F, and Naldini, L. Ensuring a Future for Gene Therapy for Rare Diseases. Nat Med (2022) 28(10):1985–8. doi:10.1038/s41591-022-01934-9
7. Salmikangas, P, Schuessler-Lenz, M, Ruiz, S, Celis, P, Reischl, I, Menezes-Ferreira, M, et al. Marketing Regulatory Oversight of Advanced Therapy Medicinal Products (ATMPs) in Europe: The EMA/CAT Perspective. Regul Aspects Gene Ther Cel Ther Prod A Glob Perspective (2015) 871:103–30. doi:10.1007/978-3-319-18618-4_6
8. Cuende, N, Ciccocioppo, R, Forte, M, Galipeau, J, Ikonomou, L, Levine, BL, et al. Patient Access to and Ethical Considerations of the Application of the European Union Hospital Exemption Rule for Advanced Therapy Medicinal Products. Cytotherapy (2022) 24(7):686–90. doi:10.1016/j.jcyt.2022.03.007
9. Salzman, R, Cook, F, Hunt, T, Malech, HL, Reilly, P, Foss-Campbell, B, et al. Addressing the Value of Gene Therapy and Enhancing Patient Access to Transformative Treatments. Mol Ther (2018) 26(12):2717–26. doi:10.1016/j.ymthe.2018.10.017
10. Sabatini, MT, Xia, T, and Chalmers, M. Pricing and Market Access Challenges in the Era of One-Time Administration Cell and Gene Therapies. Pharm Med (2022) 36(5):265–74. doi:10.1007/s40290-022-00443-x
11. Fox, T, Bueren, J, Candotti, F, Fischer, A, Aiuti, A, Lankester, A, et al. Access to Gene Therapy for Rare Diseases when Commercialization Is Not Fit for Purpose. Nat Med (2023) 29(3):518–9. doi:10.1038/s41591-023-02208-8
12. De Luca, M, and Cossu, G. Cost and Availability of Novel Cell and Gene Therapies: Can We Avoid a Catastrophic Second Valley of Death? EMBO Rep (2023) 24:e56661. doi:10.15252/embr.202256661
13. Farkas, AM, Mariz, S, Stoyanova-Beninska, V, Celis, P, Vamvakas, S, Larsson, K, et al. Advanced Therapy Medicinal Products for Rare Diseases: State of Play of Incentives Supporting Development in Europe. Front Med (2017) 4:53. doi:10.3389/fmed.2017.00053
14. Tripathy, S, and Das, SK. Strategies for Organ Preservation: Current Prospective and Challenges. Cel Biol Int (2023) 47:520–38. doi:10.1002/cbin.11984
15. Romano, M, Fanelli, G, Albany, CJ, Giganti, G, and Lombardi, G. Past, Present, and Future of Regulatory T Cell Therapy in Transplantation and Autoimmunity. Front Immunol (2019) 10:43. doi:10.3389/fimmu.2019.00043
16. Seimetz, D, Heller, K, and Richter, J. Approval of First CAR-Ts: Have We Solved All Hurdles for ATMPs? Cel Med (2019) 11:2155179018822781. doi:10.1177/2155179018822781
17. Amini, L, Kaeda, J, Fritsche, E, Roemhild, A, Kaiser, D, and Reinke, P. Clinical Adoptive Regulatory T Cell Therapy: State of the Art, Challenges, and Prospective. Front Cel Dev Biol (2022) 10:1081644. doi:10.3389/fcell.2022.1081644
18. Hennessy, C, Deptula, M, Hester, J, and Issa, F. Barriers to Treg Therapy in Europe: From Production to Regulation. Front Med (2023) 10:1090721. doi:10.3389/fmed.2023.1090721
19. Adamo, D, Attico, E, and Pellegrini, G. Education for the Translation of Advanced Therapy Medicinal Products. Front Med (2023) 10:1125892. doi:10.3389/fmed.2023.1125892
20. Silva, DN, Chrobok, M, Ahlén, G, Blomberg, P, Sällberg, M, and Pasetto, A. ATMP Development and Pre-GMP Environment in Academia: A Safety Net for Early Cell and Gene Therapy Development and Manufacturing. Immuno-Oncology Tech (2022) 16:100099. doi:10.1016/j.iotech.2022.100099
21. Medicine, AFR, Industries, EFP, Associations Bioindustries, EA, and Beattie, S. Call for More Effective Regulation of Clinical Trials with Advanced Therapy Medicinal Products Consisting of or Containing Genetically Modified Organisms in the European Union. Hum Gene Ther (2021) 32(19-20):997–1003. doi:10.1089/hum.2021.058
22. Ortíz-Maldonado, V, Rives, S, Castellà, M, Alonso-Saladrigues, A, Benítez-Ribas, D, Caballero-Baños, M, et al. CART19-BE-01: A Multicenter Trial of ARI-0001 Cell Therapy in Patients with CD19+ Relapsed/Refractory Malignancies. Mol Ther (2021) 29(2):636–44. doi:10.1016/j.ymthe.2020.09.027
23. Trias, E, Juan, M, Urbano-Ispizua, A, and Calvo, G. The Hospital Exemption Pathway for the Approval of Advanced Therapy Medicinal Products: An Underused Opportunity? the Case of the CAR-T ARI-0001. Bone Marrow Transplant (2022) 57(2):156–9. doi:10.1038/s41409-021-01463-y
24. Ivaskiene, T, Mauricas, M, and Ivaska, J. Hospital Exemption for Advanced Therapy Medicinal Products: Issue in Application in the European Union Member States. Curr Stem Cel Res Ther (2017) 12(1):45–51. doi:10.2174/1574888x11666160714114854
25. Jacobsen, S, and Svane, IM. Advanced Therapy Medicinal Products: Briefing Paper. Leuven, Belgium: The League of European Research Universities (2019).
26. Sánchez-Guijo, F, Avendaño-Solá, C, Badimón, L, Bueren, JA, Canals, JM, Delgadillo, J, et al. Role of Hospital Exemption in Europe: Position Paper from the Spanish Advanced Therapy Network (TERAV). Bone Marrow Transplant (2023) 58:727–8. doi:10.1038/s41409-023-01962-0
27. Bunnik, EM, De Jongh, D, and Massey, E. Ethics of Early Clinical Trials of Bio-Artificial Organs. Transpl Int (2022) 35:137. doi:10.3389/ti.2022.10621
28. Pearce, KF, Hildebrandt, M, Greinix, H, Scheding, S, Koehl, U, Worel, N, et al. Regulation of Advanced Therapy Medicinal Products in Europe and the Role of Academia. Cytotherapy (2014) 16(3):289–97. doi:10.1016/j.jcyt.2013.08.003
Keywords: advanced therapy medicinal products (ATMPs), regulatory processes, clinical trials, rare diseases, transplantation
Citation: Piemonti L, Scholz H, de Jongh D, Kerr-Conte J, van Apeldoorn A, Shaw JAM, Engelse MA, Bunnik E, Mühlemann M, Pal-Kutas K, Scott WE III, Magalon J, Kugelmeier P and Berishvili E (2023) The Relevance of Advanced Therapy Medicinal Products in the Field of Transplantation and the Need for Academic Research Access: Overcoming Bottlenecks and Claiming a New Time. Transpl Int 36:11633. doi: 10.3389/ti.2023.11633
Received: 31 May 2023; Accepted: 12 September 2023;
Published: 27 September 2023.
Copyright © 2023 Piemonti, Scholz, de Jongh, Kerr-Conte, van Apeldoorn, Shaw, Engelse, Bunnik, Mühlemann, Pal-Kutas, Scott, Magalon, Kugelmeier and Berishvili. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lorenzo Piemonti, cGllbW9udGkubG9yZW56b0Boc3IuaXQ=
†These authors have contributed equally to this work