 Marco Petrus Adrianus Wilhelmus Claasen1,2
Marco Petrus Adrianus Wilhelmus Claasen1,2 Dimitri Sneiders1†
Dimitri Sneiders1† Yannick Sebastiaan Rakké1†
Yannick Sebastiaan Rakké1† René Adam3Sherrie Bhoori4
René Adam3Sherrie Bhoori4 Umberto Cillo5
Umberto Cillo5 Constantino Fondevila6
Constantino Fondevila6 Maria Reig7
Maria Reig7 Gonzalo Sapisochin2Parissa Tabrizian8
Gonzalo Sapisochin2Parissa Tabrizian8 Christian Toso9* on behalf of the ESOT Guidelines Taskforce
Christian Toso9* on behalf of the ESOT Guidelines Taskforce- 1Department of Surgery, Division of HPB & Transplant Surgery, Erasmus MC Transplant Institute, University Medical Centre Rotterdam, Rotterdam, Netherlands
- 2Multi-Organ Transplant Program, University Health Network (UHN), Toronto, ON, Canada
- 3Centre Hépato-Biliaire, APHP Hôpital Universitaire Paul Brousse, Université Paris-Saclay, Paris, France
- 4Hepatology, Hepato-Pancreato-Biliary Surgery and Liver Transplantation, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy
- 5Chirurgia Generale 2, Epato-Bilio-Pancreatica e Centro Trapianto di Fegato, Azienda Ospedale Università Padova, Padova, Italy
- 6General and Digestive Surgery, University Hospital La Paz, Madrid, Spain
- 7BCLC Group, Liver Unit, Digestive Disease Institute, Hospital Clínic, IDIBAPS CIBEREHD, University of Barcelona, Barcelona, Spain
- 8Liver Transplant and Hepatobiliary Surgery, Recanati/Miller Transplantation Institute, Icahn School of Medicine at Mount Sinai, New York, NY, United States
- 9Division of Abdominal Surgery, Faculty of Medicine, University of Geneva, Geneva, Switzerland
Liver transplantation offers the best chance of cure for most patients with non-metastatic hepatocellular carcinoma (HCC). Although not all patients with HCC are eligible for liver transplantation at diagnosis, some can be downstaged using locoregional treatments such as ablation and transarterial chemoembolization. These aforementioned treatments are being applied as bridging therapies to keep patients within transplant criteria and to avoid them from dropping out of the waiting list while awaiting a liver transplant. Moreover, immunotherapy might have great potential to support downstaging and bridging therapies. To address the contemporary status of downstaging, bridging, and immunotherapy in liver transplantation for HCC, European Society of Organ Transplantation (ESOT) convened a dedicated working group comprised of experts in the treatment of HCC to review literature and to develop guidelines pertaining to this cause that were subsequently discussed and voted during the Transplant Learning Journey (TLJ) 3.0 Consensus Conference that took place in person in Prague. The findings and recommendations of the working group on Downstaging, Bridging and Immunotherapy in Liver Transplantation for Hepatocellular Carcinoma are presented in this article.
Introduction
Liver transplantation offers the best chance of cure for most patients with non-metastatic hepatocellular carcinoma (HCC). After their introduction in 1996, the Milan Criteria (a single lesion of ≤5 cm or 2–3 lesions of ≤3 cm) became the standard for patient eligibility for transplantation [1]. In later years, several expended selection criteria were introduced. Of these, the University of California San Francisco (UCSF) criteria (a single lesion of ≤6.5 cm or 2–3 lesions ≤4.5 cm with a total diameter ≤8 cm), the Up-to-seven criteria (the sum of the size of the largest tumor [in cm] and the number of tumors should not exceed 7), and the French AFP model (a score calculated based on a combination of AFP level, tumor size, and number which should not exceed 2) have been most widely accepted [2–4]. Post-transplant survival rates for patients transplanted within these established criteria exceed 70% at 5 years and 60% at 10 years [2, 3, 5–7]. To keep patients within these criteria while awaiting transplant and to avoid them from dropping out of the waiting list, bridging therapies such as ablation and transarterial chemoembolization (TACE) are being applied. Similarly, these treatments are used to downstage patients from outside established HCC transplant criteria to within these criteria, allowing them to become eligible for liver transplantation. When successful, downstaged patients can achieve equally meaningful post-transplant survival outcomes exceeding 65% at 5 years and 50% at 10 years [5, 8–10].
Although still in development and only recently added as part of the first-line treatment of patients with advanced HCC, immunotherapy too offers great potential in furthering the treatment of HCC [11]. Evidence for immunotherapy in neoadjuvant settings is already accumulating from early phase trials in various solid tumor types and also in HCC few studies have shown promising results, reporting major pathological response (≥70% necrosis) in 20%–42% of resected patients after receipt of neoadjuvant immunotherapy [12–15].
To address the contemporary status of downstaging, bridging, and the role of immunotherapy in both these strategies in the specific context of liver transplantation for HCC, ESOT convened a consensus conference, comprised of a global panel of expert hepatologists, transplant surgeons, and oncologists to develop guidelines on key aspects of Downstaging, Bridging and Immunotherapy in Liver Transplantation for Hepatocellular Carcinoma. The consensus findings and recommendations of these ESOT Consensus guidelines are presented in this document and are intended for healthcare providers.
Methods
The consensus development process was governed by a dedicated ESOT Guidelines Taskforce with support from its sections, and specifically for this work the European Liver and Intestine Transplant Association (ELITA), European Transplant Allied Healthcare Professionals (ETHAP), Education Committee, Young Professionals in Transplantation (YPT), Transplant International editorial board members and patient representatives. The detailed description of methodology used is reported previously [16].
Briefly, key issues related to Downstaging, Bridging and Immunotherapy in Liver Transplantation for HCC were identified by the working group and specific clinical questions were formulated according to the PICO methodology (PICO = Population, Intervention, Comparator and Outcome) [17]. All PICO questions are listed in Table 1 and further specified in the Supplementary Material. Following the definition of the PICOs, literature searches were developed (Supplementary Material). In some, support was provided by expert staff from the Centre for Evidence in Transplantation (CET) who have expertise in conducting systematic reviews. Search strategies differed based on the type of question and whether CET was involved or not and were conducted between 14 July 2022 and 31 October 2022.
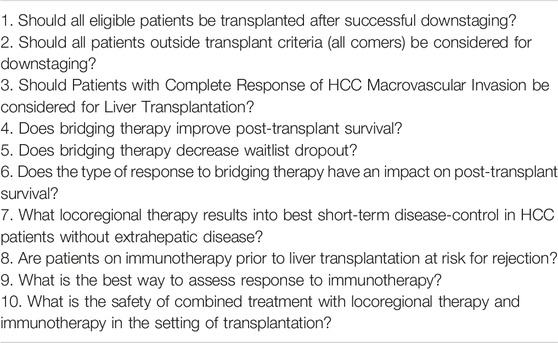
TABLE 1. Population, Intervention, Comparator and Outcome (PICO) questions.
A summary of the evidence addressing each key question by the included studies was prepared in evidence Supplementary Tables S1–S10 (Supplementary Material). The workgroup proposed a recommendation for each key question, based on the quality of evidence rated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach, with high quality rated as A, medium quality as B, and low quality as C; very low quality of evidence was not considered. For evaluation of the quality of evidence according to GRADE the following features were considered: study design, risk of bias, inconsistency, indirectness, imprecision, number of patients, effect, importance and publication bias [18]. Strength of recommendation was rated as 1 (strong) or 2 (weak).
Complete information including the list of consensus conference workgroup domains and process regarding consensus conference participant selection, development and refinement of consensus statements, are previously reported, in beforehand of the in-person conference held in Prague, Czech Republic, 13–15 November 2022 [16].
Results
1. Should all Eligible Patients Be Transplanted After Successful Downstaging?
Currently, given the scarcity of graft resources and competing indications for liver transplantation, patients beyond conventional pre-defined criteria are often not transplanted. Despite achieving successful downstaging to within accepted criteria, patients are not always offered the option of liver transplantation. The question remains whether they should.
Recommendation 1.1: All HCC patients achieving a successful downstaging to pre-defined transplantable criteria should be considered for liver transplantation as the benefit in terms of both recurrence-free survival and overall survival of this approach is significantly higher than any other non-transplant strategy.
Quality of Evidence: High.
Strength of Recommendation: Strong for.
Unmet needs: There are no specific unmet needs. Nonetheless, additional high-quality evidence could help refine, expand and/or strengthen a future recommendation on the topic.
One single reference, a 2020 randomized controlled trial by Mazzaferro et al., met the pre-defined PICO criteria and was included for review (Supplementary Table S1) [10]. This study analyzed 74 patients from nine different Italian centers and showed that after an effective and sustained downstaging of tumors originally beyond Milan criteria, liver transplantation improved tumor event-free survival and overall survival compared with non-transplantation therapies [10]. Data supporting that successfully downstaged patients should be considered for liver transplantation.
2. Should all Patients Outside Transplant Criteria (All Comers) Be Considered for Downstaging?
Many patients with HCC are diagnosed at an advanced stage, falling beyond accepted transplant criteria. However, if the overall tumor burden were to decrease, they could potentially reach a stage for which liver transplantation is usually indicated. Whether this should be actively pursued, treating patients with the goal of lowering their tumor burden so that liver transplantation might become possible, regardless of their initial stage, is still up for debate.
Recommendation 2.1: All patients beyond transplant criteria, without extra-hepatic disease or macrovascular invasion, should be considered for downstaging as long as potentially eligible for transplantation, as the original HCC state has not demonstrated to significantly hamper post-transplant survival.
Quality of Evidence: Low.
Strength of Recommendation: Strong for.
Unmet needs: There are no specific unmet needs. Nonetheless, additional higher quality evidence could help refine, expand and/or strengthen a future recommendation on the topic.
After reviewing 413 references, six observational studies were found to meet the PICO criteria (Supplementary Table S2) [5, 8, 19–21]. All these six studies showed no impact of the original HCC state on post-transplant survival. Although some studies showed a trend towards decreased disease-free survival in patients with advanced HCC (based on size and number) compared to those with less advanced HCC before downstaging, none reached significance [5, 8, 20]. In addition, one study based on waitlist alpha-fetoprotein (AFP) changes even suggested the opposite, utilizing the United States (US) Scientific Registry of Transplant Recipients (SRTR) and including 60 highly selected patients. In the cohort of patients demonstrating a waitlist AFP decrease below 400 ng/mL, those with high original AFP >1,000 ng/mL showed a trend towards better post-transplant survival compared to those with original AFP between 400 and 700, and between 700 and 100 ng/mL (100% vs. ∼75% vs. ∼55%, p = 0.072) [19]. Altogether, the identified studies support the use of downstaging in all patients with HCC beyond conventional criteria (all comers) as long as potentially eligible for transplantation, as the post-transplant survival in case of successful downstaging is not negatively influenced by the original HCC state. Of note, data suggest that a combination of morphological and biological (AFP) criteria should be used to assess the success of downstaging in all comer patients [22]. Also, enough time should be left between a successful downstaging and transplantation (e.g., >6 months) to decrease the risk of post-transplant recurrence [22].
Note: The higher the burden of disease (based on morphology and/or biology), the lower the likelihood to achieve successful downstaging.
Quality of Evidence: Moderate.
Although the original HCC state has no demonstrated impact on post-transplant survival, several studies showed that patients with advanced HCC are more likely to fail downstaging strategies, confirming the role of downstaging as a selection tool. To illustrate, two studies including 209 and 326 patients reported rates of successful downstaging to within Milan criteria at 39.1% and 38.2% for patients originally beyond UCSF criteria, and at 58% and 45.2% for patients originally between Milan and UCSF (p = 0.042, p = 0.001) [20, 23]. However, as downstaging and palliation involve similar locoregional and systemic treatments, it can generally be argued that it is to the patients’ benefit to keep them in a downstaging strategy.
3. Should Patients With Complete Response of HCC Macrovascular Invasion Be Considered for Liver Transplantation?
Macrovascular invasion has historically been a contraindication for liver transplantation in patients with HCC. Although difficult to treat, some patients with macrovascular invasion manage to achieve complete radiologic response after locoregional or systemic treatment. Whether these patients should be considered for liver transplantation is still to be answered.
Recommendation 3.1: There is insufficient evidence to recommend or not recommend liver transplantation for patients with HCC macrovascular invasion with complete response to therapy.
Quality of Evidence: Low.
Strength of Recommendation: N/A.
Unmet needs: Outcomes for patients with HCC and macrovascular invasion transplanted after complete response by pre-operative therapy are missing. Therefore, future studies should focus on neoadjuvant locoregional or systemic therapies and sustained (∼6 months) complete response. In this effort, differences in type of portal vein tumor thrombus (Vp1-Vp4) should also be compared.
Of the 85 references found, seven studies met all pre-defined PICO criteria. After reviewing their references, one more study was identified for inclusion, bringing the total to eight studies for further review (Supplementary Table S3) [24–30]. Although several studies demonstrated a 5 years overall survival rate of more than 50% in patients who received downstaging treatments before transplantation, most studies also reported high recurrence rates [24–30]. The largest included study, by Yu et al., analyzed 176 patients with portal vein tumor thrombus (PVTT) type 1–2 and showed a 5 years overall survival of 78.3% in patients with type 1 PVTT compared to 51.6% for those with type 2 PVTT (p = 0.005) [28]. However, recurrence-free survival was about 46% in both groups. Moreover, no subgroup analysis was performed for patients who achieved complete response after pre-operative therapy. This subgroup analysis was also lacking in most of the other included studies [24, 25, 29, 30]. The two studies that did report on outcomes for patients with radiologic (near-to) complete response, by Soin et al. (n = 25) and Serenari et al. (n = 5), showed a 5 years overall survival of 57% and 60%, and a recurrence rate of 24% and 60%, respectively [26, 27]. Consequently, due to insufficient evidence in the contemporary literature, no clear recommendation can be made on whether or not patients with HCC and macrovascular invasion should be considered for transplantation after complete radiologic response. If pursued, this strategy should be carried out within specific clinical trial settings.
4. Does Bridging Therapy Improve Post-Transplant Survival?
Bridging therapy is commonly used to keep patients with HCC within established transplant criteria. However, it is uncertain whether this also results in improved post-transplant survival and should therefore be standard practice for every patient on the transplant waiting list.
Recommendation 4.1: There are some studies that suggest a positive effect of bridging therapy on long-term post-transplant survival. Therefore, bridging therapy should be considered in patients if feasible.
Quality of Evidence: Low.
Strength of Recommendation: Strong for.
Unmet needs: There are no specific unmet needs. Nonetheless, additional higher quality evidence could help refine, expand and/or strengthen a future recommendation on the topic.
After screening 989 references, eight studies were selected for full review. One was a systematic review and meta-analysis (the studies analyzed herein were not separately reinstated for full review), the remaining seven were observational studies (Supplementary Table S4) [31–38]. Some of the identified studies showed significantly better long-term post-transplant survival outcomes in patients treated with bridging therapy [33, 35, 37, 38]. The largest of these studies, by Xing and Kim, looked at 14.511 transplanted patients within Milan criteria pre-transplant (3.889 with bridging, 10.622 without) and showed a 1, 3, and 5 years post-transplant survival of 95%, 85%, 80% in bridged patients versus 94%, 83%, 78% in patients without bridging (p < 0.001) [37]. In the multivariable analysis, bridging therapy remained associated with a significantly better post-transplant survival with a hazard ratio (HR) of 2.28 (95% CI 1.39–3.14; p = 0.003). Bauschke et al. showed in their cohort of 70 patients, all within Milan criteria, that the survival benefit persists even after 10 years post-transplant (95% bridged vs. 73% without bridging, p = 0.014) [33]. Another study analysing patients classified as within Milan criteria pre-transplant showed that the positive effect of bridging therapy on post-transplant survival even seems to last in a setting of recurrence, where the median survival of recurred bridged patients was 75.9 months versus 53.1 months in patients without bridging treatment (p = 0.001) [35]. Looking specifically at patients within UCSF criteria, two studies were evaluated, one with 134 patients and another with 39 patients, but both failed to report any statistical difference in survival between bridged and non-bridged patients.
5. Does Bridging Therapy Decrease Waitlist Dropout?
It is widely believed that bridging therapy is effective in keeping patients within established transplant criteria, however, whether it actually results in reduced waitlist dropout has yet to be confirmed.
Recommendation 5.1: Due to inherent confounding in the indication to bridge, evidence in the current literature is insufficient to identify whether or not bridging therapy decreases waitlist dropout. Therefore, no recommendation can be made.
Quality of Evidence: Low.
Strength of Recommendation: N/A.
Unmet needs: To determine whether bridging therapy actually results in a reduction in waitlist dropout, avoiding the currently inherited confounding in the indication to bridge, a randomized controlled trial would be required. However, with the current assumption that bridging therapy, already standard practice, is effective in keeping patients within transplant criteria, such a trial is considered ethically unjustifiable.
A total of 634 references were identified, of which six observational studies and one systematic review and meta-analysis met the pre-defined PICO criteria (the studies analyzed in the systematic review were not separately reinstated for review) (Supplementary Table S5) [31, 34, 36, 38–41]. Considering the most common transplant criteria (Milan, UCSF, ETC), none of the identified studies showed a decrease in overall or disease-specific waitlist dropout for patients who received bridging treatment compared to those without bridging treatment [31, 34, 36, 38–41]. Although not statistically significant, some of the studies did show a longer waitlist time in the group of patients who received bridging therapy [34, 36, 39, 40]. When specifically focussing on progression-related waitlist dropout, one study—evaluating 265 patients within Milan criteria—showed a statistically significantly lower dropout rate in the bridged patient population (2.58%) versus patients without bridging therapy (8.18%) [38]. However, the all-cause waitlist dropout in this study was higher in the bridged patient group (28.4% vs. 14.5% without bridging). Another study, a 2018 meta-analysis by Kulik and others, evaluating 257 cirrhotic patients classified as T2 HCC (patients within Milan criteria), reported no difference in progression-related waitlist dropout between groups treated with and without bridging treatment (relative risk [RR] 0.32; 95% confidence interval 0.06–1.85) [31]. Whether the type of bridging therapy plays a role in waitlist dropout was evaluated in the study by Györi et al., where they analyzed 84 patients within Milan criteria [34]. A transarterial chemoembolization (TACE)-based group (n = 48) was compared with a percutaneous ethanol injection (PEI)/radiofrequency ablation (RFA) group (n = 32) and a control group consisting of patients without bridging treatment (n = 22). They found no difference in all-cause waitlist dropout between groups: 41.7% TACE-based vs. 31.2% PEI/RFA vs. 36.4% control (p = 0.65) [34]. However, a serious limitation in all these retrospective studies, is the inextricable involvement of selection bias in the indication for bridging. Consequently, bridged and non-bridged populations consistently include non-comparable groups of patients and therefore ineluctably mask any effect that bridging therapy might have on waiting list dropout. Thus, precluding the effect of bridging on waitlist dropout from being inferred.
6. Does the Type of Response to Bridging Therapy Have an Impact on Post-Transplant Survival?
Bridging therapies are used in several patients within conventional transplant criteria to delay tumor progression and to minimize the risk of de-listing while on the waiting-list (dropout). Despite the strong belief that the type of response to bridging is able of influencing the rate of post-transplant tumor recurrence, this, and the weight that tumor response may have on post-transplant survival, have yet to be determined.
Recommendation 6.1: The aim of all bridging treatments carried out on the waiting-list should be to achieve a complete pathological response as this has shown to be associated with both improved recurrence-free and overall survival. Since there is no radiological imaging yet able of accurately predicting post-transplant complete pathologic response, sustained radiologic response may be considered as the best surrogate to pursue in the pre-transplant setting.
Quality of Evidence: Low.
Strength of Recommendation: Strong for.
Unmet needs: There are no specific unmet needs. Nonetheless, additional higher quality evidence could help refine, expand and/or strengthen a future recommendation on the topic.
Given the high rate of overestimation of treatment response of radiology over pathology, the literature review focused on pathologic responses only. After the identification of 423 references, nine references were included for further review (Supplementary Table S6) [35, 42–49]. All but one study analyzed outcomes achieved after both bridging and downstaging therapies, with TACE being the most commonly used treatment modality. In all studies, patients with complete pathologic response at explant pathology showed better overall survival and recurrence-free survival rates compared with those without complete pathological response [35, 42–49]. Allard et al. found that the favorable prognostic effect of response induced by TACE on explant pathology in 189 patients was confirmed not just for complete necrosis but also for “near to complete responses” (>90%), suggesting a “nearly all - or nothing” rule [48]. This data was later confirmed by the largest single-center US experience (n = 501) published by Agopian in the same year, updated in 2020 in a multicentric fashion including 3,439 patients undergoing liver transplantation from 2002 to 2013 in 20 US centers and all receiving bridging and/or downstaging therapies pre-transplant (with 802 patients showing complete pathological response) [43, 49]. All data supporting the need to pursue a complete (or close to complete) radiological tumor response in patients with HCC listed for liver transplantation.
7. What Locoregional Therapy Results Into Best Short-Term Disease-Control in HCC Patients Without Extrahepatic Disease?
Many different types of locoregional therapy for HCC exist. In the context of liver transplantation, locoregional therapy is used in the attempt to effectively control the patient’s tumor burden until a suitable liver donor becomes available for transplantation. Consequently, adequate short-term disease control is desired. What type of locoregional therapy best achieves this remains to be determined.
Recommendation 7.1: Specifically for waitlisted patients, no recommendation can be made due to the absence of unconfounded evidence. Therefore, the type of locoregional therapy should be selected according to patient and center characteristics using multidisciplinary assessment. Although data outside a transplant setting cannot be translated directly to waitlisted patients, they can provide guidance in determining which treatment might be advisable for different patients (Table 2).
Quality of Evidence: Low.
Strength of Recommendation: N/A.
Unmet needs: To determine what locoregional therapy results into best short-term disease-control in waitlisted HCC patients, avoiding both selection bias and the many patient-related confounders, randomized controlled trials would be required. However, given many patient-related and treatment-related confounders determine whether certain types of locoregional therapies can be applied to selected patients with HCC, accruing enough patients in such trials will be extremely difficult.
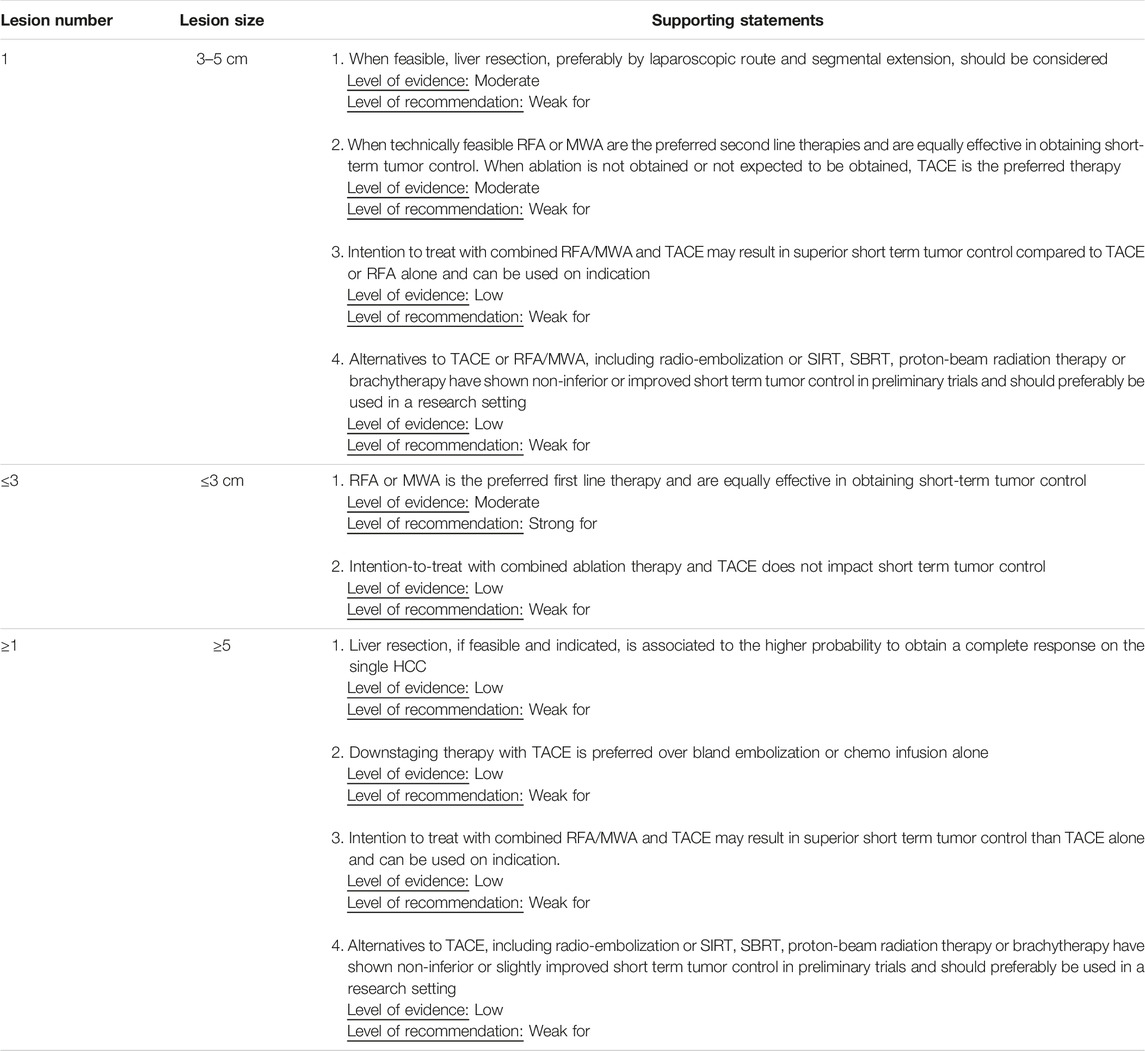
TABLE 2. Guidance document for determining the best locoregional treatment approach for short-term disease control in patients with HCC based on randomized controlled trials of locoregional treatment in a non-transplant setting.
As treatment allocation in clinical practice is subjected to both confounding factors and selection bias, only randomized controlled trials (RCTs) on the application of locoregional therapies outside a transplant setting were included. This approach allows for the least biased comparison between therapeutic modalities. Of the 2,944 unique references found, 40 RCTs comparing at least two treatment modalities were included for further review (Supplementary Table S7) [50–88]. Treatment comparisons were grouped according to lesion size and number combinations.
RCTs on uninodular lesions with size up to 3 cm (BLCL 0, A; within Milan) have compared: radiofrequency ablation (RFA) to percutaneous ethanol injection (PEI) [52, 57, 68, 74, 77], RFA to percutaneous laser ablation (PLA) [80], RFA to percutaneous acetic acid injection (PAAI) [57, 64], RFA to cryoablation [55], RFA to microwave ablation (MWA) [50, 58, 59, 69, 73, 76], and RFA to RFA combinatorial approaches [61, 65, 70, 71, 78, 82]. RFA appeared to induce higher frequencies of radiological complete responses (rCR) and improved 1 year local recurrence (LR) rate compared to PEI and PLA. Compared to PAAI, RFA induced similar rCR. However, 3 years LR rate was improved in RFA-treated versus PAAI-treated patients (RR = 0.41, 95% CI: 023–0.91) [57]. Cryoablation has been shown to have equal rCR, 1 year LR rate, 1-year overall survival, and 1 year disease-free survival as RFA, albeit in a single RCT [55]. In a meta-analysis on RCTs among RFA- and MWA-treated lesions no difference in radiological complete response rates was observed (RR: 1.01, 95% CI: 0.99–1.02) [67]. Moreover, 1 year disease-free and overall survival rates were similar. No difference in adverse events (Aes) could be observed between RFA and MWA-treated patients. RCTs on combination of RFA with TACE [65, 70, 82] or other therapeutic regimen (PEI [71], Iodine-125 [78], Interferon alpha [61]) did not show or report any difference in rCR in these tumor lesions compared to RFA only.
RCTs comparing RFA to PEI [52, 74], RFA to PLA [80], RFA to PAAI [64], RFA to cryoablation [55], and RFA to MWA [50, 58, 59, 69, 73, 76] have included uninodular lesions, ranging 3–5 cm as well. As RFA and MWA in these trials have shown to be clinically effective one might suggest that these techniques are preferred as first line regimen. Yet, locoregional ablative therapies tend to become less effective if tumor lesion size increases.
In case of increased tumor burden, intra-arterial therapies or radiotherapy provide an alternative. Different RCTs on uninodular lesions ranging 3–5 cm (BCLC A; within Milan) and uni-/multinodular lesions ≥5 cm (BCLC A, outside Milan; BCLC B, outside Milan, resp.) have compared: TACE to transarterial or “bland” embolization (TAE) [54, 60, 81, 84], TACE/RFA to TACE combined with RFA [51, 56, 65, 66, 70, 72, 86], TACE to transarterial radio-embolization (TARE) [53, 62, 83, 88], TACE to transarterial ethanol ablation (TAEA) [75], TACE to transarterial chemo-infusion (TACI) [63], and TACE to radiotherapy [79, 85]. Hyperselective TACE (tend to) induced higher frequencies of rCR or radiological partial response (rPR) compared to “bland” embolization. 1 year disease-free and overall survival was either non-significantly different among the groups or tended to be increased in TACE-treated patients. When combining TACE with ablative therapies, combination regimen appeared to induce higher rCR (i.e., + PEI [66], + RFA [86], and + cryoablation [51]), 1 year disease-free survival [66], and 1-year overall survival [51, 86], although studied in relatively small cohorts. RCTs comparing TACE to TARE have shown conflicting results. Whereas Raoul et al. reported no difference in rCR/PR when using Iodine-131 radioembolisation [53], other trials have shown a trend to higher radiological response rates in Yttrium-90 (Y-90) radioembolization cohorts compared to TACE [83, 88]. Moreover, Salem et al. have observed that Y-90 appeared to have lower 1 year LR rate [62]. Generally, treatment-related or grade ≥3 AEs were either equal or reduced in favor of TARE. Conformably, in the prospective, multi-center, non-randomized MERITS-LT trial both TACE and Y90-TARE showed equal efficacy in downstaging towards liver transplantation [87]. Though not statistically significant, explanted livers of TARE-treated patients demonstrated higher frequencies of tumor necrosis (30.8% vs. 20.5%) and lower frequencies microvascular invasion (7.7% vs. 20.5%) hinting towards improved local tumor control. Nowadays, TARE has been accepted as an effective alternative in case TACE is contraindicated (e.g., portal thrombosis). To this end, no clear benefit of TAEA, TACI, or radiotherapy (i.e., proton-beam, brachytherapy) over TACE in RCTs was observed. Yet, recent prospective cohort studies strongly hint to safe and superior efficacy of stereotactic body radiotherapy over TACE as bridge to transplant [89, 90]. Any conclusive results on these therapies are expected from ongoing phase III RCTs (i.e., NCT03960008).
Although this data provides valuable insight in the potential of each locoregional treatment in a non-transplant setting, their results cannot directly be translated to waitlisted patients. Therefore, no recommendations can be made. Nonetheless, these comparisons can provide guidance in determining the kind of treatment to pursue (Table 2).
8. Are Patients on Immunotherapy Prior to Liver Transplantation at Risk for Rejection?
Immunotherapy has recently become part of the standard treatment for advanced unresectable HCC who are not amenable to curative or locoregional therapy. Due to its promising results, interest has emerged in the use of immunotherapy in a neoadjuvant setting. Whether patients receiving immunotherapy prior to liver transplantation are at risk for rejection has yet to be determined.
Recommendation 8.1: Due to insufficient evidence, no meaningful recommendation can be made.
Quality of Evidence: Low.
Strength of Recommendation: N/A.
Unmet needs: (1) Further investigations are needed to explore the safety and long-term oncologic outcomes in the pre-transplant setting. (2) Patient selection for immune checkpoint inhibitors (ICI), minimal washout period between the last drug dose and transplantation, observation period, biomarkers are unmet clinical needs that require investigation.
Of the 1,560 references identified, nine studies on liver transplantation in patients previously treated with immune checkpoint inhibitors were included, representing 27 cases (Supplementary Table S8) [91–99]. The first case reported resulted in fatal hepatic necrosis at day 8th and patient loss [91]. The ICI was given within 4 weeks before transplantation. A minimum washout period (4 weeks) prior to transplantation given the half-life of 27 days was proposed. Subsequent reports have shown successful results [92, 94–99]. In total, four cases of severe rejection were reported with two successful re-transplantations [91, 93, 97, 98]. Since drug type, pre-transplant treatment and dosage, tumor burden, and response vary from case to case, further investigations are needed to explore the safety and long term oncologic outcomes in a pre-transplant setting.
9. What is the Best Way to Assess Response to Immunotherapy?
To optimize the use of immunotherapy treatment in patients with HCC and to be able to evaluate its effect in a (neo)adjuvant setting, it is imperative that tumor response after immunotherapy can be adequately assessed. However, the best way to do this has yet to be determined.
Recommendation 9.1: There is insufficient evidence to make any meaningful recommendation on how best to assess response to immunotherapy for HCC.
Quality of Evidence: Low.
Strength of Recommendation: N/A.
Unmet needs: (1) Improved imaging techniques and biomarkers are needed to define response ahead of pathologic assessment and oncologic outcomes. (2) Explant analysis of specimens should be done prospectively with careful radiology-pathology correlation.
After an extensive review of 6,800 references, seven studies were selected for inclusion (Supplementary Table S9) [11, 13–15, 100–102]. Radiologic evaluation of response after immunotherapy is primarily derived from the recent trials on immunotherapy within advanced HCC where survival benefit was associated with objective response and significant reduction in tumor burden [11, 100–102]. In these studies, the objective response rate by mRECIST ranged from 22% to 34%, whereas complete response was reported in 2.2%–5.5% of the cases [11, 100–102]. Unfortunately, these studies lack confirmation of actual response through pathological assessment. Three recent trials that published on the use of neoadjuvant therapy prior to resection in HCC did report on both response seen on imaging and determined by pathologic assessment. Complete pathologic response ranged from 8% to 25% and major pathologic response (>70% necrosis) was seen in 20%–42%, while pre-operative imaging according to RECIST 1.1 reported partial and complete response in only 8%–15% and 0%, respectively [13–15]. Although data on imaging-pathology response correlations in a transplantation setting are lacking, encouraging pathologic response rates have been reported. In a study of 9 patients who underwent ICI in combination with locoregional therapy, downstaging was successful in 4/5 patients and major pathologic response (>70% necrosis) was noted in 6/9 patients [96]. Improved imaging techniques and biomarkers are needed to define response ahead of pathologic assessment and oncologic outcomes. Given the high rate of explants exceeding Milan criteria post transplantation, significant limitations occur with the current contrast enhanced computed tomography (CT) and magnetic resonance imaging techniques (MRI) in predicting treatment response [87]. In addition, with the use of immunotherapies, the immunologic changes within the tumor and tumor microenvironment may impact the relation between the degree of pathologic and radiographic response [14]. Moreover, the vasoconstrictive and antiangiogenic effects of the drugs may induce a false positive assessment of response by mRECIST [103, 104].
10. What Is the Safety of Combined Treatment With Locoregional Therapy and Immunotherapy in the Setting of Transplantation?
A combined treatment of immunotherapy and locoregional therapy may be more effective than each treatment separately. However, it remains to be seen whether such combined treatment approach is safe in the context of transplantation.
Recommendation 10.1: Since there is no data in the context of pre- or post-liver transplantation, no recommendation can be made.
Quality of Evidence: N/A.
Strength of Recommendation: N/A.
Unmet needs: Further investigations that explore the safety and long-term oncologic outcomes in the pre- and post-transplant setting are needed.
Since no data was found on combined treatment with locoregional and immunotherapy in the setting of transplantation, data outside transplant setting was assessed. In this context, a total of 450 references were identified, whereas 14 were eventually included for further review (Supplementary Table S10) [105–119]. Two of these were systematic reviews and meta-analyses [105, 106]. The first, including 19 studies and comparing TACE or RFA with immunotherapy, did not evaluate safety profiles [105]. The second, including four studies comparing TACE with dendritic cells therapy, reported that patients in the TACE-DC-CIK group were more likely to suffer a fever than the ones in the control group (p = 0.001). In the five prospective studies, one randomized controlled trial and four non-randomized trials, no safety difference between arms was reported [110–115]. However, the small sample sizes limited the robustness of their conclusion. Finally, of the seven non-randomized retrospective studies, five focused on early-death or severe complications with none of the studies reporting any major complication or death associated with the treatment evaluated [108, 117–120]. In the remaining two retrospective studies safety was not reported [107, 109]. Although these data provide valuable insight into the safety and long-term oncologic outcomes of combined treatments of locoregional therapy and immunotherapy in a non-transplant setting, they cannot be extrapolated to a transplant/waitlist-setting. Therefore, no recommendation can be made.
Summary and Future Considerations
The Transplant Learning Journey (TLJ) 3.0 consensus conference resulted in several recommendations pertaining to Downstaging, Bridging and Immunotherapy in Liver Transplantation for HCC. Starting with downstaging. Though not always successful, downstaging should always be aimed for regardless of disease burden as the original HCC state has demonstrated little impact on post-transplant survival. Moreover, as downstaging and palliation involve similar locoregional and systemic treatments, it can generally be argued that it is to the patients’ benefit to keep them in a downstaging strategy. If successful downstaging has been achieved, patients should always be considered for liver transplantation as the benefit in terms of both recurrence-free and overall survival of this approach is significantly higher than any other non-transplant strategy. Although liver transplantation for patients with macrovascular invasion has been shown to be feasible, recurrence rates are generally high, necessitating further investigation to determine whether patients with HCC and macrovascular invasion should be considered for liver transplantation if complete radiologic response has been achieved. In the context of bridging, some studies suggest a positive effect of bridging therapy on long-term post-transplant survival and therefore should be considered if feasible. When applied, the aim should be to attain complete response, as a complete pathological response has shown to be associated with improved recurrence-free and overall survival. Since radiological imaging is not able to accurately predict post-transplant complete pathologic response, sustained radiologic response may be considered as the best surrogate to pursue in the pre-transplant setting. Unfortunately, whether or not bridging therapy decreases waitlist dropout cannot be determined from the contemporary literature due to inherent confounding in the indication to bridge. In terms of the type of bridging therapy to use, selection should be made according to patient and center characteristics using multidisciplinary assessment. Finally, although immunotherapy has shown promising results, further investigations are needed to explore its safety (rejection) and long-term oncologic outcomes in a pre-transplant setting, as well as which patients to select, the minimal washout period between the last drug dose and transplantation, and the optimal duration of observance. The same holds for immunotherapy use in a pre- or post-transplant setting when combined with locoregional treatments. To support research in these areas, improved imaging techniques and biomarkers are needed to define immunotherapeutic response ahead of pathologic assessment and oncologic outcomes.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author Contributions
Involved in the conception or design of the work: MC, DS, YR, RA, SB, UC, CF, MR, GS, PT, and CT. Literature screen and review: MC, DS, YR, RA, SB, UC, CF, MR, GS, PT, and CT. Drafted the article: MC, DS, YR, RA, SB, UC, CF, MR, GS, PT, and CT. Critically revised the article: MC, DS, YR, RA, SB, UC, CF, MR, GS, PT, and CT. Finally approved the version to be published: MC, DS, YR, RA, SB, UC, CF, MR, GS, PT, and CT. All authors contributed to the article and approved the submitted version.
Collaborators
Helena Degroote (Department of Hepatology and Gastroenterology, Ghent University Hospital, Belgium); Andrea Della Penna, Silvio Nadalin (Department of General, Visceral and Transplant Surgery, University Hospital Tübingen, Tübingen, Germany); Emmanouil Giorgakis (Division of Transplantation, Department of Surgery, University of Arkansas for Medical Sciences, Little Rock, AR, United States); Oleg Godik (Department of Pediatric Surgery & Urology, National Medical University and Clinic Oberig, Kiev, Ukraine); Mihnea-ioan Ionescu (The Liver Unit, Queen Elizabeth Hospital Birmingham, University Hospitals Birmingham NHS Foundation Trust, Birmingham, United Kingdom); Giulia Magini (Division of Abdominal Surgery, Faculty of Medicine, University of Geneva, Geneva, Switzerland); Wojtek Polak (Department of Surgery, Division of HPB & Transplant Surgery, Erasmus MC Transplant Institute, University Medical Centre Rotterdam, Rotterdam, Netherlands); Karen Rockell (Co-Director and PPIE Lead of the UK Organ Donation and Transplantation Research Network, London, United Kingdom); Gianluca Rompianesi (Department of Clinical Medicine and Surgery, Federico II University Hospital, Naples, Italy); Ian Rowe (Leeds Institute for Medical Research, University of Leeds, Leeds, United Kingdom); Stratigoula Sakellariou (First Department of Pathology, National and Kapodistrian University of Athens, Laiko General Hospital, Athens, Greece); Katharina Staufer (Department of Internal Medicine III, Division of Gastroenterology & Hepatology, Medical University of Vienna, Austria; Department of General Surgery, Division of Transplantation, Medical University of Vienna, Austria); Luca Toti (HPB and Transplant Unit, Department of Surgery, University of Rome Tor Vergata, Rome, Italy).
Funding
All costs related to taskforce and workgroup meetings were covered by ESOT, without external funding.
Conflict of Interest
GS discloses consultancy for AstraZeneca, Roche, Novartis, Evidera and Integra. GS has received financial compensation for talks for Roche, AstraZeneca, Chiesi, and Integra. GS has received a grant from Roche. PT discloses consultancy for/receipt of honorarium from Bayer, Boston Scientific, and Aztrazeneca. MR discloses consultancy/advisory role for AstraZeneca, Bayer, BMS, Eli Lilly, Geneos, Ipsen, Merck, Roche, Universal DX, and Boston. MR has received funding from ISCIII and CIBER. MR has given talks for AstraZeneca, Bayer, BMS, Eli Lilly, Gilead, and Roche. MR’s institution has received grant research support from Bayer and Ipsen, and educational support from Astrazeneca, Bayer, Roche, Eisai, Ipsen, Lilly, and Terumo. UC discloses Astellas (Travel Grants & Advisory Board), Eisai (Advisory Board), MSD (Advisory Board), Novartis (Consultant, Travel Grants & Advisory Board), Pfizer (Travel Grants), Sandoz (Advisory Board), Sanofi (Consultant), Springer Healthcare (Copyright & Advisory Board), and J&J (Consultant, Travel Grants). SB discloses talks and has an advisory role for AstraZeneca, Ipsen, MSD, Roche, Eisai, Terumo and Boston Scientific.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This manuscript and the ESOT Consensus Working Group is a collaborative work product of ESOT and its Sections and Committees. We would like to thank Devi Mey, Justyna Klimek, Irene Garcia, Giovanna Rossi, Daniele Roppolo and the entire ESOT staff for their tireless efforts to support this endeavor. We would also like to thank Liset Pengel, the CET and the YPTs for coordinating and performing literature searches which were additionally instrumental in this endeavor.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontierspartnerships.org/articles/10.3389/ti.2023.11648/full#supplementary-material
References
1. Mazzaferro, V, Regalia, E, Doci, R, Andreola, S, Pulvirenti, A, Bozzetti, F, et al. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N Engl J Med (1996) 334(11):693–9. doi:10.1056/NEJM199603143341104
2. Yao, FY, Ferrell, L, Bass, NM, Watson, JJ, Bacchetti, P, Venook, A, et al. Liver Transplantation for Hepatocellular Carcinoma: Expansion of the Tumor Size Limits Does Not Adversely Impact Survival. Hepatology (2001) 33(6):1394–403. doi:10.1053/jhep.2001.24563
3. Mazzaferro, V, Llovet, JM, Miceli, R, Bhoori, S, Schiavo, M, Mariani, L, et al. Predicting Survival after Liver Transplantation in Patients with Hepatocellular Carcinoma beyond the Milan Criteria: A Retrospective, Exploratory Analysis. Lancet Oncol (2009) 10(1):35–43. doi:10.1016/S1470-2045(08)70284-5
4. Duvoux, C, Roudot-Thoraval, F, Decaens, T, Pessione, F, Badran, H, Piardi, T, et al. Liver Transplantation for Hepatocellular Carcinoma: A Model Including α-fetoprotein Improves the Performance of milan Criteria. Gastroenterology (2012) 143(4):985–6. doi:10.1053/j.gastro.2012.05.052
5. Tabrizian, P, Holzner, ML, Mehta, N, Halazun, K, Agopian, VG, Yao, F, et al. Ten-Year Outcomes of Liver Transplant and Downstaging for Hepatocellular Carcinoma. JAMA Surg (2022) 157:779–88. doi:10.1001/jamasurg.2022.2800
6. Barreto, SG, Strasser, SI, McCaughan, GW, Fink, MA, Jones, R, McCall, J, et al. Expansion of Liver Transplantation Criteria for Hepatocellular Carcinoma from Milan to UCSF in Australia and New Zealand and Justification for Metroticket 2.0. Cancers (Basel) (2022) 14(11):2777. doi:10.3390/cancers14112777
7. Notarpaolo, A, Layese, R, Magistri, P, Gambato, M, Colledan, M, Magini, G, et al. Validation of the AFP Model as a Predictor of HCC Recurrence in Patients with Viral Hepatitis-Related Cirrhosis Who Had Received a Liver Transplant for HCC. J Hepatol (2017) 66(3):552–9. doi:10.1016/j.jhep.2016.10.038
8. Ahmed, O, Vachharajani, N, Croome, KP, Tabrizian, P, Agopian, V, Halazun, K, et al. Are Current National Review Board Downstaging Protocols for Hepatocellular Carcinoma Too Restrictive? J Am Coll Surg (2022) 234(4):579–88. doi:10.1097/XCS.0000000000000140
9. Mehta, N, Guy, J, Frenette, CT, Dodge, JL, Osorio, RW, Minteer, WB, et al. Excellent Outcomes of Liver Transplantation Following Down-Staging of Hepatocellular Carcinoma to within Milan Criteria: A Multicenter Study. Clin Gastroenterol Hepatol (2018) 16(6):955–64. doi:10.1016/j.cgh.2017.11.037
10. Mazzaferro, V, Citterio, D, Bhoori, S, Bongini, M, Miceli, R, De Carlis, L, et al. Liver Transplantation in Hepatocellular Carcinoma after Tumour Downstaging (XXL): A Randomised, Controlled, Phase 2b/3 Trial. Lancet Oncol (2020) 21(7):947–56. doi:10.1016/S1470-2045(20)30224-2
11. Finn, RS, Qin, S, Ikeda, M, Galle, PR, Ducreux, M, Kim, TY, et al. Atezolizumab Plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med (2020) 382(20):1894–905. doi:10.1056/nejmoa1915745
12. Pinato, DJ, Fessas, P, Sapisochin, G, and Marron, TU. Perspectives on the Neoadjuvant Use of Immunotherapy in Hepatocellular Carcinoma. Hepatology (2021) 74(1):483–90. doi:10.1002/hep.31697
13. Kaseb, AO, Hasanov, E, Cao, HST, Xiao, L, Vauthey, JN, Lee, SS, et al. Perioperative Nivolumab Monotherapy versus Nivolumab Plus Ipilimumab in Resectable Hepatocellular Carcinoma: A Randomised, Open-Label, Phase 2 Trial. Lancet Gastroenterol Hepatol (2022) 7(3):208–18. doi:10.1016/S2468-1253(21)00427-1
14. Ho, WJ, Zhu, Q, Durham, J, Popovic, A, Xavier, S, Leatherman, J, et al. Neoadjuvant Cabozantinib and Nivolumab Converts Locally Advanced HCC into Resectable Disease with Enhanced Antitumor Immunity. Nat Cancer (2021) 2(9):891–903. doi:10.1038/s43018-021-00234-4
15. Marron, TU, Fiel, MI, Hamon, P, Fiaschi, N, Kim, E, Ward, SC, et al. Neoadjuvant Cemiplimab for Resectable Hepatocellular Carcinoma: A Single-Arm, Open-Label, Phase 2 Trial. Lancet Gastroenterol Hepatol (2022) 7(3):219–29. doi:10.1016/S2468-1253(21)00385-X
16. Cillo, U, Weissenbacher, A, Pengel, L, Jochmans, I, Roppolo, D, Amarelli, C, et al. ESOT Consensus Platform for Organ Transplantation: Setting the Stage for a Rigorous, Regularly Updated Development Process. Transpl Int (2022) 35:10915. doi:10.3389/ti.2022.10915
17. Davies, KS. Formulating the Evidence Based Practice Question: A Review of the Frameworks. Evid Based Libr Inf Pract (2011) 6(2):75–80. doi:10.18438/b8ws5n
18. Guyatt, GH, Oxman, AD, Vist, GE, Kunz, R, Falck-Ytter, Y, Alonso-Coello, P, et al. GRADE: An Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations. Bmj (2008) 336(7650):924–6. doi:10.1136/bmj.39489.470347.AD
19. Merani, S, Majno, P, Kneteman, NM, Berney, T, Morel, P, Mentha, G, et al. The Impact of Waiting List Alpha-Fetoprotein Changes on the Outcome of Liver Transplant for Hepatocellular Carcinoma. J Hepatol (2011) 55(4):814–9. doi:10.1016/j.jhep.2010.12.040
20. Chapman, WC, Garcia-Aroz, S, Vachharajani, N, Fowler, K, Saad, N, Lin, Y, et al. Liver Transplantation for Advanced Hepatocellular Carcinoma after Downstaging without Up-Front Stage Restrictions. J Am Coll Surg (2017) 224(4):610–21. doi:10.1016/j.jamcollsurg.2016.12.020
21. Murali, AR, Romero-Marrero, C, Miller, C, Aucejo, F, Levitin, A, Gill, A, et al. Predictors of Successful Downstaging of Hepatocellular Carcinoma outside Milan Criteria. Criteria Transplant (2016) 100(11):2391–7. doi:10.1097/TP.0000000000001402
22. Mehta, N, Dodge, JL, Grab, JD, and Yao, FY. National Experience on Down-Staging of Hepatocellular Carcinoma before Liver Transplant: Influence of Tumor Burden, Alpha-Fetoprotein, and Wait Time. Hepatology (2020) 71(3):943–54. doi:10.1002/hep.30879
23. Degroote, H, Piñero, F, Costentin, C, Notarpaolo, A, Boin, IF, Boudjema, K, et al. International Study on the Outcome of Locoregional Therapy for Liver Transplant in Hepatocellular Carcinoma beyond Milan Criteria. JHEP Rep (2021) 3(5):100331. doi:10.1016/j.jhepr.2021.100331
24. Assalino, M, Terraz, S, Grat, M, Lai, Q, Vachharajani, N, Gringeri, E, et al. Liver Transplantation for Hepatocellular Carcinoma after Successful Treatment of Macrovascular Invasion – a Multi-center Retrospective Cohort Study. Transpl Int (2020) 33(5):567–75. doi:10.1111/tri.13586
25. Han, DH, Joo, DJ, Kim, MS, Choi, GH, Choi, JS, Park, YN, et al. Living Donor Liver Transplantation for Advanced Hepatocellular Carcinoma with portal Vein Tumor Thrombosis after Concurrent Chemoradiation Therapy. Yonsei Med J (2016) 57(5):1276–81. doi:10.3349/ymj.2016.57.5.1276
26. Serenari, M, Cappelli, A, Cucchetti, A, Mosconi, C, Strigari, L, Monari, F, et al. Deceased Donor Liver Transplantation after Radioembolization for Hepatocellular Carcinoma and Portal Vein Tumoral Thrombosis: A Pilot Study. Liver Transpl (2021) 27(12):1758–66. doi:10.1002/lt.26257
27. Soin, AS, Bhangui, P, Kataria, T, Baijal, SS, Piplani, T, Gautam, D, et al. Experience with LDLT in Patients with Hepatocellular Carcinoma and portal Vein Tumor Thrombosis Postdownstaging. Transplantation (2020) 104(11):2334–45. doi:10.1097/TP.0000000000003162
28. Yu, J, Zhuang, L, Liu, P, Liu, Z, Ling, S, Deng, Y, et al. Long-term Outcomes of Deceased Donor Liver Transplantation in Hepatocellular Carcinoma Patients with portal Vein Tumor Thrombus: A Multicenter Study. Eur J Surg Oncol (2022) 48(1):121–32. doi:10.1016/j.ejso.2021.08.014
29. Bhatti, ABH, Naqvi, W, Khan, NY, Zia, HH, Dar, FS, Khan, ZA, et al. Living Donor Liver Transplantation for Advanced Hepatocellular Carcinoma Including Macrovascular Invasion. J Cancer Res Clin Oncol (2022) 148(1):245–53. doi:10.1007/s00432-021-03665-9
30. Lv, JY, Zhang, NN, Du, YW, Wu, Y, Song, TQ, Zhang, YM, et al. Comparison of Liver Transplantation and Liver Resection for Hepatocellular Carcinoma Patients with portal Vein Tumor Thrombus Type I and Type II. Yonsei Med J (2021) 62(1):29–40. doi:10.3349/ymj.2021.62.1.29
31. Kulik, L, Heimbach, JK, Zaiem, F, Almasri, J, Prokop, LJ, Wang, Z, et al. Therapies for Patients with Hepatocellular Carcinoma Awaiting Liver Transplantation: A Systematic Review and Meta-Analysis. Hepatology (2018) 67(1):381–400. doi:10.1002/hep.29485
32. Al Sebayel, MI, Elsiesy, H, Al-Hamoudi, W, Alabbad, S, Elsheikh, Y, Elbeshbeshy, H, et al. Effect of Downstaging and Bridging of Hepatocellular Carcinoma on Survival Following Liver Transplant: A Single center Experience. Exp Clin Transpl (2017) 15:7–11. doi:10.6002/ect.TOND16.L4
33. Bauschke, A, Altendorf-Hofmann, A, Ardelt, M, Kissler, H, Tautenhahn, HM, and Settmacher, U. Impact of Successful Local Ablative Bridging Therapy Prior to Liver Transplantation on Long-Term Survival in Patients with Hepatocellular Carcinoma in Cirrhosis. J Cancer Res Clin Oncol (2020) 146(7):1819–27. doi:10.1007/s00432-020-03215-9
34. Györi, GP, Felsenreich, DM, Silberhumer, GR, Soliman, T, and Berlakovich, GA. Multimodality Locoregional Treatment Strategies for Bridging HCC Patients before Liver Transplantation. Eur Surg - Acta Chir Austriaca (2017) 49(5):236–43. doi:10.1007/s10353-017-0487-8
35. Oligane, HC, Xing, M, and Kim, HS. Effect of Bridging Local-Regional Therapy on Recurrence of Hepatocellular Carcinoma and Survival after Orthotopic Liver Transplantation. Radiology (2017) 282(3):869–79. doi:10.1148/radiol.2016160288
36. Tan, CHN, Yu, Y, Tan, YRN, Lim, BLK, Iyer, SG, Madhavan, K, et al. Bridging Therapies to Liver Transplantation for Hepatocellular Carcinoma: A Bridge to Nowhere? Ann Hepato-biliary-pancreatic Surg (2018) 22(1):27–35. doi:10.14701/ahbps.2018.22.1.27
37. Xing, M, and Kim, HS. Independent Prognostic Factors for Posttransplant Survival in Hepatocellular Carcinoma Patients Undergoing Liver Transplantation. Cancer Med (2017) 6(1):26–35. doi:10.1002/cam4.936
38. Xing, M, Sakaria, S, Dhanasekaran, R, Parekh, S, Spivey, J, Knechtle, SJ, et al. Bridging Locoregional Therapy Prolongs Survival in Patients Listed for Liver Transplant with Hepatocellular Carcinoma. Cardiovasc Intervent Radiol (2017) 40(3):410–20. doi:10.1007/s00270-016-1505-0
39. Aravinthan, AD, Bruni, SG, Doyle, AC, Thein, HH, Goldaracena, N, Issachar, A, et al. Liver Transplantation Is a Preferable Alternative to Palliative Therapy for Selected Patients with Advanced Hepatocellular Carcinoma. Ann Surg Oncol (2017) 24(7):1843–51. doi:10.1245/s10434-017-5789-3
40. Lai, Q, Vitale, A, Iesari, S, Finkenstedt, A, Mennini, G, Onali, S, et al. The Intention-To-Treat Effect of Bridging Treatments in the Setting of Milan Criteria–In Patients Waiting for Liver Transplantation. Liver Transpl (2019) 25(7):1023–33. doi:10.1002/lt.25492
41. Habibollahi, P, Hunt, S, Gade, T, Dagli, MS, Mondschein, JI, Sudheendra, D, et al. The Impact of Bridging LRT on Survival in Patients Listed for Liver Transplantation. Cardiovasc Intervent Radiol (2018) 41(1):112–9. doi:10.1007/s00270-017-1759-1
42. Majno, PE, Adam, R, Bismuth, H, Castaing, D, Ariche, A, Krissat, J, et al. Influence of Preoperative Transarterial Lipiodol Chemoembolization on Resection and Transplantation for Hepatocellular Carcinoma in Patients with Cirrhosis. Ann Surg (1997) 226(6):688–701. doi:10.1097/00000658-199712000-00006
43. Agopian, VG, Morshedi, MM, McWilliams, J, Harlander-Locke, MP, Markovic, D, Zarrinpar, A, et al. Complete Pathologic Response to Pretransplant Locoregional Therapy for Hepatocellular Carcinoma Defines Cancer Cure after Liver Transplantation: Analysis of 501 Consecutively Treated Patients. Ann Surg (2015) 262(3):536–45. doi:10.1097/SLA.0000000000001384
44. Cantù, M, Piardi, T, Sommacale, D, Ellero, B, Woehl-Jaegle, ML, Audet, M, et al. Pathologic Response to Non-surgical Locoregional Therapies as Potential Selection Criteria for Liver Transplantation for Hepatocellular Carcinoma. Ann Transpl (2013) 18(1):273–84. doi:10.12659/AOT.883939
45. Ravaioli, M, Grazi, GL, Ercolani, G, Fiorentino, M, Cescon, M, Golfieri, R, et al. Partial Necrosis on Hepatocellular Carcinoma Nodules Facilitates Tumor Recurrence after Liver Transplantation. Transplantation (2004) 78(12):1780–6. doi:10.1097/01.tp.0000145892.97114.ee
46. Bharat, A, Brown, DB, Crippin, JS, Gould, JE, Lowell, JA, Shenoy, S, et al. Pre-Liver Transplantation Locoregional Adjuvant Therapy for Hepatocellular Carcinoma as a Strategy to Improve Longterm Survival. J Am Coll Surg (2006) 203(4):411–20. doi:10.1016/j.jamcollsurg.2006.06.016
47. Manzia, TM, Lai, Q, Iesari, S, Perera, MTPR, Komuta, M, Carvalheiro, A, et al. Impact of Remnant Vital Tissue after Locoregional Treatment and Liver Transplant in Hepatocellular Cancer Patients, a Multicentre Cohort Study. Transpl Int (2018) 31(9):988–98. doi:10.1111/tri.13153
48. Allard, MA, Sebagh, M, Ruiz, A, Guettier, C, Paule, B, Vibert, E, et al. Does Pathological Response after Transarterial Chemoembolization for Hepatocellular Carcinoma in Cirrhotic Patients with Cirrhosis Predict Outcome after Liver Resection or Transplantation? J Hepatol (2015) 63(1):83–92. doi:10.1016/j.jhep.2015.01.023
49. DiNorcia, J, Florman, SS, Haydel, B, Tabrizian, P, Ruiz, RM, Klintmalm, GB, et al. Pathologic Response to Pretransplant Locoregional Therapy Is Predictive of Patient Outcome after Liver Transplantation for Hepatocellular Carcinoma: Analysis from the US Multicenter HCC Transplant Consortium. Ann Surg (2020) 271(4):616–24. doi:10.1097/SLA.0000000000003253
50. Vietti Violi, N, Duran, R, Guiu, B, Cercueil, JP, Aubé, C, Digklia, A, et al. Efficacy of Microwave Ablation versus Radiofrequency Ablation for the Treatment of Hepatocellular Carcinoma in Patients with Chronic Liver Disease: A Randomised Controlled Phase 2 Trial. Lancet Gastroenterol Hepatol (2018) 3(5):317–25. doi:10.1016/S2468-1253(18)30029-3
51. Huang, C, Zhuang, W, Feng, H, Guo, H, Tang, Y, Chen, H, et al. Analysis of Therapeutic Effectiveness and Prognostic Factor on Argon-Helium Cryoablation Combined with Transcatheter Arterial Chemoembolization for the Treatment of Advanced Hepatocellular Carcinoma. J Cancer Res Ther (2016) 12:C148–52. doi:10.4103/0973-1482.200605
52. Lencioni, RA, Allgaier, HP, Cioni, D, Olschewski, M, Deibert, P, Crocetti, L, et al. Small Hepatocellular Carcinoma in Cirrhosis: Randomized Comparison of Radio-Frequency thermal Ablation versus Percutaneous Ethanol Injection. Radiology (2003) 228(1):235–40. doi:10.1148/radiol.2281020718
53. Raoul, JL, Guyader, D, Bretagne, JF, Heautot, JF, Duvauferrier, R, Bourguet, P, et al. Prospective Randomized Trial of Chemoembolization versus Intra-arterial Injection of 131I-Labeled-Iodized Oil in the Treatment of Hepatocellular Carcinoma. Hepatology (1997) 26(5):1156–61. doi:10.1002/hep.510260511
54. Meyer, T, Kirkwood, A, Roughton, M, Beare, S, Tsochatzis, E, Yu, D, et al. A Randomised Phase II/III Trial of 3-weekly Cisplatin-Based Sequential Transarterial Chemoembolisation vs Embolisation Alone for Hepatocellular Carcinoma. Br J Cancer (2013) 108(6):1252–9. doi:10.1038/bjc.2013.85
55. Wang, C, Wang, H, Yang, W, Hu, K, Xie, H, Hu, KQ, et al. Multicenter Randomized Controlled Trial of Percutaneous Cryoablation versus Radiofrequency Ablation in Hepatocellular Carcinoma. Hepatology (2015) 61(5):1579–90. doi:10.1002/hep.27548
56. El-Kady, NM, Esmat, G, Mahmoud, EH, Darweesh, SK, Mahmoud, SH, and Elagawy, WA. Hypertonic saline-enhanced Radiofrequency versus Chemoembolization Sequential Radiofrequency in the Treatment of Large Hepatocellular Carcinoma. Eur J Gastroenterol Hepatol (2013) 25(5):628–33. doi:10.1097/MEG.0b013e32835d2c4f
57. Lin, SM, Lin, CJ, Lin, CC, Hsu, CW, and Chen, YC. Randomised Controlled Trial Comparing Percutaneous Radiofrequency thermal Ablation, Percutaneous Ethanol Injection, and Percutaneous Acetic Acid Injection to Treat Hepatocellular Carcinoma of 3 Cm or Less. Gut (2005) 54(8):1151–6. doi:10.1136/gut.2004.045203
58. Shibata, T, Iimuro, Y, Yamamoto, Y, Maetani, Y, Ametani, F, Itoh, K, et al. Small Hepatocellular Carcinoma: Comparison of Radio-Frequency Ablation and Percutaneous Microwave Coagulation Therapy. Radiology (2002) 223(2):331–7. doi:10.1148/radiol.2232010775
59. Chong, CCN, Lee, KF, Cheung, SYS, Chu, CCM, Fong, AKW, Wong, J, et al. Prospective Double-Blinded Randomized Controlled Trial of Microwave versus RadioFrequency Ablation for Hepatocellular Carcinoma (McRFA Trial). HPB (2020) 22(8):1121–7. doi:10.1016/j.hpb.2020.01.008
60. Brown, KT, Do, RK, Gonen, M, Covey, AM, Getrajdman, GI, Sofocleous, CT, et al. Randomized Trial of Hepatic Artery Embolization for Hepatocellular Carcinoma Using Doxorubicin-Eluting Microspheres Compared with Embolization with Microspheres Alone. J Clin Oncol (2016) 34(17):2046–53. doi:10.1200/JCO.2015.64.0821
61. Kalra, N, Kang, M, Duseja, AK, Bhatia, A, Singh, V, Dhiman, RK, et al. Comparison of Radiofrequency Ablation Alone & in Combination with Percutaneous Ethanol Injection for Management of Hepatocellular Carcinoma. Indian J Med Res (2017) 146:S30–7. doi:10.4103/ijmr.IJMR_1812_15
62. Salem, R, Gordon, AC, Mouli, S, Hickey, R, Kallini, J, Gabr, A, et al. Y90 Radioembolization Significantly Prolongs Time to Progression Compared with Chemoembolization in Patients with Hepatocellular Carcinoma. Gastroenterology (2016) 151(6):1155–63. doi:10.1053/j.gastro.2016.08.029
63. Okusaka, T, Kasugai, H, Shioyama, Y, Tanaka, K, Kudo, M, Saisho, H, et al. Transarterial Chemotherapy Alone versus Transarterial Chemoembolization for Hepatocellular Carcinoma: A Randomized Phase III Trial. J Hepatol (2009) 51(6):1030–6. doi:10.1016/j.jhep.2009.09.004
64. Paul, SB, Acharya, SK, Gamanagatti, SR, Sreenivas, V, Shalimar, S, and Gulati, MS. Acetic Acid versus Radiofrequency Ablation for the Treatment of Hepatocellular Carcinoma: A Randomized Controlled Trial. Diagn Interv Imaging (2020) 101(2):101–10. doi:10.1016/j.diii.2019.06.011
65. Peng, ZW, Zhang, YJ, Chen, MS, Xu, L, Liang, HH, Lin, XJ, et al. Radiofrequency Ablation with or without Transcatheter Arterial Chemoembolization in the Treatment of Hepatocellular Carcinoma: A Prospective Randomized Trial. J Clin Oncol (2013) 31(4):426–32. doi:10.1200/JCO.2012.42.9936
66. Bartolozzi, C, Lencioni, R, Caramella, D, Vignali, C, Cioni, R, Mazzeo, S, et al. Treatment of Large HCC: Transcatheter Arterial Chemoembolization Combined with Percutaneous Ethanol Injection versus Repeated Transcatheter Arterial Chemoembolization. Radiology (1995) 197(3):812–8. doi:10.1148/radiology.197.3.7480761
67. Facciorusso, A, Abd El Aziz, MA, Tartaglia, N, Ramai, D, Mohan, BP, Cotsoglou, C, et al. Microwave Ablation versus Radiofrequency Ablation for Treatment of Hepatocellular Carcinoma: A Meta-Analysis of Randomized Controlled Trials. Cancers (Basel) (2020) 12(12):3796. doi:10.3390/cancers12123796
68. Shiina, S, Teratani, T, Obi, S, Sato, S, Tateishi, R, Fujishima, T, et al. A Randomized Controlled Trial of Radiofrequency Ablation with Ethanol Injection for Small Hepatocellular Carcinoma. Gastroenterology (2005) 129(1):122–30. doi:10.1053/j.gastro.2005.04.009
69. Kamal, A, Elmoety, AAA, Rostom, YAM, Shater, MS, and Lashen, SA. Percutaneous Radiofrequency versus Microwave Ablation for Management of Hepatocellular Carcinoma: A Randomized Controlled Trial. J Gastrointest Oncol (2019) 10(3):562–71. doi:10.21037/jgo.2019.01.34
70. Yi, Y, Zhang, Y, Wei, Q, Zhao, L, Han, J, Song, Y, et al. Radiofrequency Ablation or Microwave Ablation Combined with Transcatheter Arterial Chemoembolization in Treatment of Hepatocellular Carcinoma by Comparing with Radiofrequency Ablation Alone. Chin J Cancer Res (2014) 26(1):112–8. doi:10.3978/j.issn.1000-9604.2014.02.09
71. Lin, SM, Lin, CJ, Hsu, CW, Tai, DI, Sheen, IS, Lin, DY, et al. Prospective Randomized Controlled Study of Interferon-Alpha in Preventing Hepatocellular Carcinoma Recurrence after Medical Ablation Therapy for Primary Tumors. Cancer (2004) 100(2):376–82. doi:10.1002/cncr.20004
72. Morimoto, M, Numata, K, Kondou, M, Nozaki, A, Morita, S, and Tanaka, K. Midterm Outcomes in Patients with Intermediate-Sized Hepatocellular Carcinoma: A Randomized Controlled Trial for Determining the Efficacy of Radiofrequency Ablation Combined with Transcatheter Arterial Chemoembolization. Cancer (2010) 116(23):5452–60. doi:10.1002/cncr.25314
73. Abdelaziz, A, Elbaz, T, Shousha, HI, Mahmoud, S, Ibrahim, M, Abdelmaksoud, A, et al. Efficacy and Survival Analysis of Percutaneous Radiofrequency versus Microwave Ablation for Hepatocellular Carcinoma: An Egyptian Multidisciplinary Clinic Experience. Surg Endosc (2014) 28(12):3429–34. doi:10.1007/s00464-014-3617-4
74. Lin, SM, Lin, CJ, Lin, CC, Hsu, CW, and Chen, YC. Radiofrequency Ablation Improves Prognosis Compared with Ethanol Injection for Hepatocellular Carcinoma < or =4 Cm. Gastroenterology (2004) 127(6):1714–23. doi:10.1053/j.gastro.2004.09.003
75. Yu, SC, Hui, JW, Hui, EP, Chan, SL, Lee, KF, Mo, F, et al. Unresectable Hepatocellular Carcinoma: Randomized Controlled Trial of Transarterial Ethanol Ablation versus Transcatheter Arterial Chemoembolization. Radiology (2014) 270(2):607–20. doi:10.1148/radiol.13130498
76. Yu, J, Yu, XL, Han, ZY, Cheng, ZG, Liu, FY, Zhai, HY, et al. Percutaneous Cooled-Probe Microwave versus Radiofrequency Ablation in Early-Stage Hepatocellular Carcinoma: A Phase III Randomised Controlled Trial. Gut (2017) 66(6):1172–3. doi:10.1136/gutjnl-2016-312629
77. Brunello, F, Veltri, A, Carucci, P, Pagano, E, Ciccone, G, Moretto, P, et al. Radiofrequency Ablation versus Ethanol Injection for Early Hepatocellular Carcinoma: A Randomized Controlled Trial. Scand J Gastroenterol (2008) 43(6):727–35. doi:10.1080/00365520701885481
78. Chen, K, Chen, G, Wang, H, Li, H, Xiao, J, Duan, X, et al. Increased Survival in Hepatocellular Carcinoma with Iodine-125 Implantation Plus Radiofrequency Ablation: A Prospective Randomized Controlled Trial. J Hepatol (2014) 61(6):1304–11. doi:10.1016/j.jhep.2014.07.026
79. Bush, DA, Smith, JC, Slater, JD, Volk, ML, Reeves, ME, Cheng, J, et al. Randomized Clinical Trial Comparing Proton Beam Radiation Therapy with Transarterial Chemoembolization for Hepatocellular Carcinoma: Results of an Interim Analysis. Int J Radiat Oncol Biol Phys (2016) 95(1):477–82. doi:10.1016/j.ijrobp.2016.02.027
80. Orlacchio, A, Bolacchi, F, Chegai, F, Bergamini, A, Costanzo, E, Del Giudice, C, et al. Comparative Evaluation of Percutaneous Laser and Radiofrequency Ablation in Patients with HCC Smaller Than 4 Cm. Radiol Med (2014) 119(5):298–308. doi:10.1007/s11547-013-0339-y
81. Llovet, JM, Real, MI, Montana, X, Planas, R, Coll, S, Aponte, J, et al. Arterial Embolisation or Chemoembolisation versus Symptomatic Treatment in Patients with Unresectable Hepatocellular Carcinoma: A Randomised Controlled Trial. Lancet (2002) 359(9319):1734–9. doi:10.1016/S0140-6736(02)08649-X
82. Shibata, T, Isoda, H, Hirokawa, Y, Arizono, S, Shimada, K, and Togashi, K. Small Hepatocellular Carcinoma: Is Radiofrequency Ablation Combined with Transcatheter Arterial Chemoembolization More Effective Than Radiofrequency Ablation Alone for Treatment? Radiology (2009) 252(3):905–13. doi:10.1148/radiol.2523081676
83. Pitton, MB, Kloeckner, R, Ruckes, C, Wirth, GM, Eichhorn, W, Worns, MA, et al. Randomized Comparison of Selective Internal Radiotherapy (SIRT) versus Drug-Eluting Bead Transarterial Chemoembolization (DEB-TACE) for the Treatment of Hepatocellular Carcinoma. Cardiovasc Interv Radiol (2015) 38(2):352–60. doi:10.1007/s00270-014-1012-0
84. Malagari, K, Pomoni, M, Kelekis, A, Pomoni, A, Dourakis, S, Spyridopoulos, T, et al. Prospective Randomized Comparison of Chemoembolization with Doxorubicin-Eluting Beads and bland Embolization with BeadBlock for Hepatocellular Carcinoma. Cardiovasc Interv Radiol (2010) 33(3):541–51. doi:10.1007/s00270-009-9750-0
85. Mohnike, K, Steffen, IG, Seidensticker, M, Hass, P, Damm, R, Peters, N, et al. Radioablation by Image-Guided (HDR) Brachytherapy and Transarterial Chemoembolization in Hepatocellular Carcinoma: A Randomized Phase II Trial. Cardiovasc Interv Radiol (2019) 42(2):239–49. doi:10.1007/s00270-018-2127-5
86. Yang, P, Liang, M, Zhang, Y, and Shen, B. Clinical Application of a Combination Therapy of Lentinan, Multi-Electrode RFA and TACE in HCC. Adv Ther (2008) 25(8):787–94. doi:10.1007/s12325-008-0079-x
87. Mehta, N, Frenette, C, Tabrizian, P, Hoteit, M, Guy, J, Parikh, N, et al. Downstaging Outcomes for Hepatocellular Carcinoma: Results from the Multicenter Evaluation of Reduction in Tumor Size before Liver Transplantation (MERITS-LT) Consortium. Gastroenterology (2021) 161(5):1502–12. doi:10.1053/j.gastro.2021.07.033
88. Kolligs, FT, Bilbao, JI, Jakobs, T, Inarrairaegui, M, Nagel, JM, Rodriguez, M, et al. Pilot Randomized Trial of Selective Internal Radiation Therapy vs. Chemoembolization in Unresectable Hepatocellular Carcinoma. Liver Int (2015) 35(6):1715–21. doi:10.1111/liv.12750
89. Sapisochin, G, Barry, A, Doherty, M, Fischer, S, Goldaracena, N, Rosales, R, et al. Stereotactic Body Radiotherapy vs. TACE or RFA as a Bridge to Transplant in Patients with Hepatocellular Carcinoma. An Intention-To-Treat Analysis. J Hepatol (2017) 67(1):92–9. doi:10.1016/j.jhep.2017.02.022
90. Wong, TC, Lee, VH, Law, AL, Pang, HH, Lam, KO, Lau, V, et al. Prospective Study of Stereotactic Body Radiation Therapy for Hepatocellular Carcinoma on Waitlist for Liver Transplant. Hepatology (2021) 74(5):2580–94. doi:10.1002/hep.31992
91. Nordness, MF, Hamel, S, Godfrey, CM, Shi, C, Johnson, DB, Goff, LW, et al. Fatal Hepatic Necrosis after Nivolumab as a Bridge to Liver Transplant for HCC: Are Checkpoint Inhibitors Safe for the Pretransplant Patient? Am J Transpl (2020) 20(3):879–83. doi:10.1111/ajt.15617
92. Schwacha-Eipper, B, Minciuna, I, Banz, V, and Dufour, JF. Immunotherapy as a Downstaging Therapy for Liver Transplantation. Hepatology (2020) 72(4):1488–90. doi:10.1002/hep.31234
93. Chen, GH, Wang, GB, Huang, F, Qin, R, Yu, XJ, Wu, RL, et al. Pretransplant Use of Toripalimab for Hepatocellular Carcinoma Resulting in Fatal Acute Hepatic Necrosis in the Immediate Postoperative Period. Transpl Immunol (2021) 66:101386. doi:10.1016/j.trim.2021.101386
94. Qiao, ZY, Zhang, ZJ, Lv, ZC, Tong, H, Xi, ZF, Wu, HX, et al. Neoadjuvant Programmed Cell Death 1 (PD-1) Inhibitor Treatment in Patients with Hepatocellular Carcinoma before Liver Transplant: A Cohort Study and Literature Review. Front Immunol (2021) 12:653437. doi:10.3389/fimmu.2021.653437
95. Sogbe, M, López-Guerra, D, Blanco-Fernández, G, Sangro, B, and Narváez-Rodriguez, I. Durvalumab as a Successful Downstaging Therapy for Liver Transplantation in Hepatocellular Carcinoma: The Importance of a Washout Period. Transplantation (2021) 105(12):E398–400. doi:10.1097/TP.0000000000003855
96. Tabrizian, P, Florman, SS, and Schwartz, ME. PD-1 Inhibitor as Bridge Therapy to Liver Transplantation? Am J Transpl (2021) 21(5):1979–80. doi:10.1111/ajt.16448
97. Schnickel, GT, Fabbri, K, Hosseini, M, Misel, M, Berumen, J, Parekh, J, et al. Liver Transplantation for Hepatocellular Carcinoma Following Checkpoint Inhibitor Therapy with Nivolumab. Am J Transpl (2022) 22(6):1699–704. doi:10.1111/ajt.16965
98. Dehghan, Y, Schnickel, GT, Hosseini, M, Burgoyne, AM, Ajmera, VH, Morris, GP, et al. Rescue Liver Re-transplantation after Graft Loss Due to Severe Rejection in the Setting of Pre-transplant Nivolumab Therapy. Clin J Gastroenterol (2021) 14(6):1718–24. doi:10.1007/s12328-021-01521-4
99. Aby, ES, and Lake, JR. Immune Checkpoint Inhibitor Therapy before Liver Transplantation - Case and Literature Review. Transpl Direct (2022) 8(4):E1304. doi:10.1097/txd.0000000000001304
100. Yau, T, Kang, YK, Kim, TY, El-Khoueiry, AB, Santoro, A, Sangro, B, et al. Efficacy and Safety of Nivolumab Plus Ipilimumab in Patients with Advanced Hepatocellular Carcinoma Previously Treated with Sorafenib: The CheckMate 040 Randomized Clinical Trial. JAMA Oncol (2020) 6(11):e204564. doi:10.1001/jamaoncol.2020.4564
101. Abou-Alfa, GK, Chan, SL, Furuse, J, Galle, PR, Kelley, RK, Qin, S, et al. A Randomized, Multicenter Phase 3 Study of Durvalumab (D) and Tremelimumab (T) as First-Line Treatment in Patients with Unresectable Hepatocellular Carcinoma (HCC): HIMALAYA Study. J Clin Oncol (2018) 36:TPS4144. doi:10.1200/jco.2018.36.15_suppl.tps4144
102. Finn, RS, Ryoo, BY, Merle, P, Kudo, M, Bouattour, M, Lim, HY, et al. Pembrolizumab as Second-Line Therapy in Patients with Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J Clin Oncol (2020) 38(3):193–202. doi:10.1200/JCO.19.01307
103. Tran, NH, Muñoz, S, Thompson, S, Hallemeier, CL, and Bruix, J. Hepatocellular Carcinoma Downstaging for Liver Transplantation in the Era of Systemic Combined Therapy with Anti-VEGF/TKI and Immunotherapy. Hepatology (2022) 76(4):1203–18. doi:10.1002/hep.32613
104. Bruix, J, Reig, M, and Sangro, B. Assessment of Treatment Efficacy in Hepatocellular Carcinoma: Response Rate, Delay in Progression or None of Them. J Hepatol (2017) 66(6):1114–7. doi:10.1016/j.jhep.2017.02.032
105. Ding, M, Wang, Y, Chi, J, Wang, T, Tang, X, Cui, D, et al. Is Adjuvant Cellular Immunotherapy Essential after TACE-Predominant Minimally-Invasive Treatment for Hepatocellular Carcinoma? A Systematic Meta-Analysis of Studies Including 1774 Patients. Sun B, Editor. PLoS One (2016) 11(12):e0168798. doi:10.1371/journal.pone.0168798
106. He, G, Zheng, C, Huo, H, Zhang, H, Zhu, Z, Li, J, et al. TACE Combined with Dendritic Cells and Cytokine-Induced Killer Cells in the Treatment of Hepatocellular Carcinoma: A Meta-Analysis. Int Immunopharmacol (2016) 40:436–42. doi:10.1016/j.intimp.2016.09.015
107. Marinelli, B, Cedillo, M, Pasik, SD, Charles, D, Murthy, S, Patel, RS, et al. Safety and Efficacy of Locoregional Treatment during Immunotherapy with Nivolumab for Hepatocellular Carcinoma: A Retrospective Study of 41 Interventions in 29 Patients. J Vasc Interv Radiol (2020) 31(11):1729–38. doi:10.1016/j.jvir.2020.07.009
108. Zhang, JX, Chen, P, Liu, S, Zu, QQ, Shi, HB, and Zhou, CG. Safety and Efficacy of Transarterial Chemoembolization and Immune Checkpoint Inhibition with Camrelizumab for Treatment of Unresectable Hepatocellular Carcinoma. J Hepatocell Carcinoma (2022) 9:265–72. doi:10.2147/JHC.S358658
109. Smith, WH, Ru, M, McGee, HM, Sung, M, Rosenzweig, KE, and Buckstein, M. Safety of Nivolumab in Combination with Prior or Concurrent Radiation Therapy in Hepatocellular Carcinoma. J Radiat Oncol (2020) 9(1–2):45–52. doi:10.1007/s13566-020-00419-x
110. de la Torre-Aláez, M, Matilla, A, Varela, M, Iñarrairaegui, M, Reig, M, Lledó, JL, et al. Nivolumab after Selective Internal Radiation Therapy for the Treatment of Hepatocellular Carcinoma: A Phase 2, Single-Arm Study. J Immunother Cancer (2022) 10(11):e005457. doi:10.1136/jitc-2022-005457
111. de la Torre-Alaez, M, Matilla, A, Varela, M, Iñarrairaegui, M, Reig, M, Luis Lledo, J, et al. Nivolumab after Selective Internal Radiation Therapy (Sirt) Using Sir-Spheres Resin Microspheres in Patients with Hepatocellular Carcinoma: The Nasir-Hcc Trial. In: International Liver Cancer Association (ILCA) Annual Conference 2020 Book of Abstracts (2020). Abstract O-27.
112. Zhang, S, Zhao, Y, He, L, Bo, C, An, Y, Li, N, et al. Effect of Camrelizumab Plus Transarterial Chemoembolization on Massive Hepatocellular Carcinoma. Clin Res Hepatol Gastroenterol (2022) 46(4):101851. doi:10.1016/j.clinre.2021.101851
113. Cui, J, Wang, N, Zhao, H, Jin, H, Wang, G, Niu, C, et al. Combination of Radiofrequency Ablation and Sequential Cellular Immunotherapy Improves Progression-free Survival for Patients with Hepatocellular Carcinoma. Int J Cancer (2014) 134(2):342–51. doi:10.1002/ijc.28372
114. Duffy, AG, Ulahannan, SV, Makorova-Rusher, O, Rahma, O, Wedemeyer, H, Pratt, D, et al. Tremelimumab in Combination with Ablation in Patients with Advanced Hepatocellular Carcinoma. J Hepatol (2017) 66(3):545–51. doi:10.1016/j.jhep.2016.10.029
115. Zhao, GS, Liu, S, Liu, Y, Li, C, Wang, RY, Bian, J, et al. Clinical Application of Gelatin Sponge Microparticles-Transcatheter Arterial Chemoembolization Combined with Synchronous Antigen-Presenting Dendritic Cell Sequential Reinfusion for Treatment of Advanced Large Liver Cancer: A single-center, Prospective, Non-randomized, Controlled Trial. Medicine (Baltimore) (2022) 101(8):e28803. doi:10.1097/MD.0000000000028803
116. Theodoro, V, de Oliveira Fujii, L, Lucke, LD, Bortolazzo, FO, Silva, DFD, Carneiro, GD, et al. Inhibitory Effect of Red LED Irradiation on Fibroblasts and Co-culture of Adipose-Derived Mesenchymal Stem Cells. Heliyon (2020) 6(5):e03882. doi:10.1016/j.heliyon.2020.e03882
117. Alnaggar, M, Lin, M, Mesmar, A, Liang, S, Qaid, A, Xu, K, et al. Allogenic Natural Killer Cell Immunotherapy Combined with Irreversible Electroporation for Stage IV Hepatocellular Carcinoma: Survival Outcome. Cell Physiol Biochem (2018) 48(5):1882–93. doi:10.1159/000492509
118. Zhan, C, Ruohoniemi, D, Shanbhogue, KP, Wei, J, Welling, TH, Gu, P, et al. Safety of Combined Yttrium-90 Radioembolization and Immune Checkpoint Inhibitor Immunotherapy for Hepatocellular Carcinoma. J Vasc Interv Radiol (2020) 31(1):25–34. doi:10.1016/j.jvir.2019.05.023
119. Guo, Y, Ren, Y, Chen, L, Sun, T, Zhang, W, Sun, B, et al. Transarterial Chemoembolization Combined with Camrelizumab for Recurrent Hepatocellular Carcinoma. BMC Cancer (2022) 22(1):270. doi:10.1186/s12885-022-09325-6
120. Huang, ZM, Li, W, Li, S, Gao, F, Zhou, QM, Wu, FM, et al. Cytokine-induced Killer Cells in Combination with Transcatheter Arterial Chemoembolization and Radiofrequency Ablation for Hepatocellular Carcinoma Patients. J Immunother (2013) 36(5):287–93. doi:10.1097/CJI.0b013e3182948452
Glossary
AE adverse events
AFP alpha-fetoprotein
CET Centre for Evidence in Transplantation
CT computed tomography
DFS disease-free survival
ELITA European Liver and Intestine Transplant Association
ESOT European Society of Organ Transplantation
ETHAP European Transplant Allied Healthcare Professionals
GRADE Grading of Recommendations Assessment, Development and Evaluation
HCC hepatocellular carcinoma
HR hazard ratio
LR local recurrence
LT liver transplantation
MRI magnetic resonance imaging
MWA microwave ablation
N/A not applicable
OS overall survival
PAAI percutaneous acetic acid injection
PEI percutaneous ethanol injection
PICO Population, Intervention, Comparator and Outcome
PLA percutaneous laser ablation
ICI immune checkpoint inhibitors
PVTT portal vein tumor thrombus
rCR radiological complete response
RCT randomized controlled trial
RFA radiofrequency ablation
RFS recurrence-free survival
rPR radiological partial response
RR relative risk
SRTR Scientific Registry of Transplant Recipients
TACE transarterial chemoembolization
TACI transarterial chemo-infusion
TAE transarterial embolization
TAEA transarterial ethanol ablation
TARE transarterial radio-embolization
TLJ Transplant Learning Journey
UCSF University of California San Francisco
US United States
Y-90 Yttrium-90
YPT Young Professionals in Transplantation
Keywords: hepatocellular carcinoma, liver transplantation, downstaging, bridging, immunotherapy
Citation: Claasen MPAW, Sneiders D, Rakké YS, Adam R, Bhoori S, Cillo U, Fondevila C, Reig M, Sapisochin G, Tabrizian P and Toso C (2023) European Society of Organ Transplantation (ESOT) Consensus Report on Downstaging, Bridging and Immunotherapy in Liver Transplantation for Hepatocellular Carcinoma. Transpl Int 36:11648. doi: 10.3389/ti.2023.11648
Received: 04 June 2023; Accepted: 22 August 2023;
Published: 14 September 2023.
Copyright © 2023 Claasen, Sneiders, Rakké, Adam, Bhoori, Cillo, Fondevila, Reig, Sapisochin, Tabrizian and Toso. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christian Toso, Y2hyaXN0aWFuLnRvc29AaGN1Z2UuY2g=
†These authors have contributed equally to this work