 Emmanouil Giorgakis1*
Emmanouil Giorgakis1* Martha M. Estrada1Allison Wells1Mauricio Garcia Saenz de Sicilia2Matthew Deneke2Raj Patel1Gary Barone1Lyle Burdine1Mary K. Rude2
Martha M. Estrada1Allison Wells1Mauricio Garcia Saenz de Sicilia2Matthew Deneke2Raj Patel1Gary Barone1Lyle Burdine1Mary K. Rude2- 1Division of Solid Organ Transplantation, Department of Surgery, University of Arkansas for Medical Sciences, Little Rock, AR, United States
- 2Division of Gastroenterology and Hepatology, Department of Medicine, University of Arkansas for Medical Sciences, Little Rock, AR, United States
Dear Editors,
Liver transplantation is the standard of care for end-stage liver disease (ESLD) and transplant oncology patients. Given the organ shortage, equitable organ distribution is key. Recent studies have repeatedly reported that, in the US, waitlisted patients of female sex are less likely to be transplanted and more likely to die awaiting a liver transplant [1, 2]. This has been largely attributed to an imperfect model for end-stage liver disease (MELD) scoring systems and donor-recipient size mismatch [1, 3, 4].
After obtaining institutional board review exemption (IRB 275415), we explored socioeconomic and sex-related disparities of patients referred for liver transplant at Arkansas’ single liver transplant institution. The Centers for Disease Control and Prevention (CDC)/Agency for Toxic Substances and Disease Registry (ATCSDR) Social Vulnerability Index (SVI) was employed as surrogate indicator of socioeconomic status [5]. Social vulnerability refers to the resilience of a population when confronted by a health stressor, be it a disease outbreak or a natural or human-caused disaster. CDC/ATSDR SVI database “can help communities prepare for and recover from public health emergencies, and prevent adverse effects among socially vulnerable populations, such as emotional distress, loss of property, illness, and death” [5]. The SVI calculation encompasses parameters reflecting a community’s socioeconomic (e.g., poverty, unemployment, per capita income, education, and health insurance), population (e.g., children or elderly, disability, single parent, minority, limited English), and housing/transportation (e.g., mobile homes, crowding, no vehicle, living in group quarters) vulnerability. Data was sourced from the Arkansas Clinical Data Repository.
Patients with less than 1 year follow-up or missing data were excluded. SVI scores were assigned by patient’s ZIP code, which reflects the patient’s location of residence. The patients were split into SVI quartiles, based on SVI median and interquartile range. Logistic regression was performed for enlisting, adjusted for SVI quartile, age, sex, body mass index, and insurance payor. A Fine-Gray survival model was built, with liver transplant as the primary outcome and death a competing event controlled for sex, SVI quartile, and insurance. Analyses were conducted using R software (4.1.0) and STATA version (17.0).
Study period was from 1st January 2019 to 31st December 2022. The study population included N = 779 patients who had been referred to our center during that time for liver transplant evaluation. 43.2% (N = 336) of these patients were female. Logistic regression analysis indicated that, irrespective of SVI quartile, male sex and private insurance were independent predictors favoring liver transplantation (odds ratio [OR] 2.73; 95% CI, 1.70–4.52, and 2.2; 95% CI, 1.35–3.70, respectively; Table 1). Likewise, on Fine-Gray analysis adjusted for SVI quartile, male sex and Medicare/Medicaid insurance payor were independent risk factors (OR 2.38; 95% CI, 1.53–3.70, and 0.48; 95% CI, 0.30–0.76, respectively) (Table 2). Waitlisted male patients with private insurance were more likely to get transplanted and survive after a liver transplant. What is more, male sex patients referred for liver transplant were found more likely to be evaluated (OR 1.76, p < 0.001), enlisted (OR 2.07, p < 0.001) and transplanted (OR 2.55, p < 0.001) compared to their female counterparts (Supplementary Data).
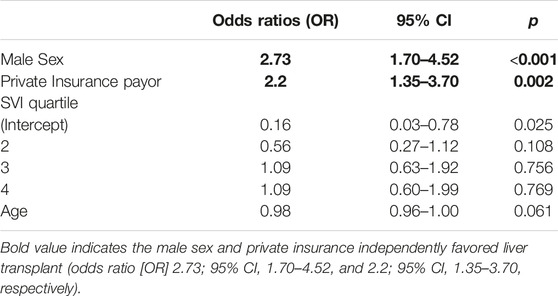
TABLE 1. Multivariate analysis of liver transplant outcome.
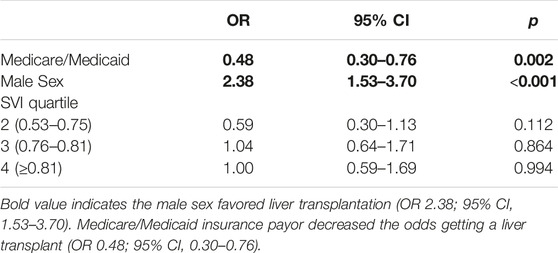
TABLE 2. Fine gray competing risk survival analysis of patients referred for liver transplant.
In conclusion, our study indicates that, in the population and period studied, there are sex related barriers in the liver transplant process. These obstacles may prevent female sex patients from entering and completing liver transplant evaluation. This gap may be ascribed to functional status assessment barriers [2], e.g., higher perceived frailty among females, particularly elderly; clinical, e.g., higher female prevalence of nonalcoholic steatohepatitis (NASH), with NASH known to be associated with higher surgical risk; social [1, 2], e.g., work or family obligations preventing completion of the evaluation process; the stigma of alcohol excess [1, 2]; or geographic, i.e., within minority groups residing in remote locations. Beyond introducing remedies such as scoring system upgrades accounting for patient’s sex [1, 2], it is also necessary to address sex-based barriers presenting early on in the liver transplant referral and evaluation process [2]. A good start may be the 1) creation of national or regional liver disease/ESLD registries in order to achieve better data granularity; 2) introduction of transplant referral and evaluation efficiency metrics (e.g., time from referral to decision over enlisting) [2]; 3) implementation of objective frailty testing methods [2]; and 4) provisions for a more flexible evaluation process, tailored to individual socioeconomic, geographic, and cultural needs.
Limitations of this pilot study were its limited sample, retrospective nature, and the inclusion of liver transplant referrals to a single US transplant institution.
Data Availability Statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving humans were approved by UAMS Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author Contributions
Conceptualization, EG and MR; methodology, EG and AW; software, EG and AW; formal analysis, AW; data curation, EG and AW; writing-original draft preparation, EG; writing-review and editing, EG, ME, LB, RP, MG, MD, GB, and MR; visualization, EG; supervision, EG. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontierspartnerships.org/articles/10.3389/ti.2023.11667/full#supplementary-material
Abbreviations
ATCDR, agency for toxic substances and disease registry; CDC, centers for disease control and prevention; ESLD, end-stage liver disease; MELD, model for end-stage liver disease; NASH, non-alcoholic steatohepatitis; SVI, social vulnerability index.
References
1. Nephew, LD, and Serper, M. Racial, Gender, and Socioeconomic Disparities in Liver Transplantation. Liver Transpl (2021) 27(6):900–12. doi:10.1002/lt.25996
2. Sawinski, D, Lai, J, Pinney, S, Gray, AL, Jackson, AM, Stewart, D, et al. Addressing Sex-Based Disparities in Solid Organ Transplantation in the United States-A Conference Report. Am J Transplant (2023) 23:316–25. doi:10.1016/j.ajt.2022.11.008
3. Locke, JE, Shelton, BA, Olthoff, KM, Pomfret, EA, Forde, KA, Sawinski, D, et al. Quantifying Sex-Based Disparities in Liver Allocation. JAMA Surg (2020) 155(7):e201129. doi:10.1001/jamasurg.2020.1129
4. Allen, AM, Heimbach, JK, Larson, JJ, Mara, KC, Kim, WR, Kamath, PS, et al. Reduced Access to Liver Transplantation in Women: Role of Height, MELD Exception Scores, and Renal Function Underestimation. Transplantation (2018) 102(10):1710–6. doi:10.1097/TP.0000000000002196
5. CDC/ATSDR. CDC/ATSDR Social Vulnerability Index (2023). Available From: https://www.atsdr.cdc.gov/placeandhealth/svi/index.html (Accessed September 7, 2023).
Keywords: disparities, liver transplant, social vulnerability index, sex disparities, public policy
Citation: Giorgakis E, Estrada MM, Wells A, Garcia Saenz de Sicilia M, Deneke M, Patel R, Barone G, Burdine L and Rude MK (2023) Women Referred for Liver Transplant Are Less Likely to Be Transplanted Irrespective of Socioeconomic Status. Transpl Int 36:11667. doi: 10.3389/ti.2023.11667
Received: 09 June 2023; Accepted: 23 October 2023;
Published: 02 November 2023.
Copyright © 2023 Giorgakis, Estrada, Wells, Garcia Saenz de Sicilia, Deneke, Patel, Barone, Burdine and Rude. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emmanouil Giorgakis, ZWdpb3JnYWtpc0B1YW1zLmVkdQ==