 Caroline Stenman1
Caroline Stenman1 Andreas Wallinder1,2Erik Holmberg3,4Kristjan Karason1,5,6
Andreas Wallinder1,2Erik Holmberg3,4Kristjan Karason1,5,6 Jesper Magnusson1,7,6Göran Dellgren1,2,6*
Jesper Magnusson1,7,6Göran Dellgren1,2,6*- 1Transplant Institute, Sahlgrenska University Hospital, Gothenburg, Sweden
- 2Department Cardiothoracic Surgery, Sahlgrenska University Hospital, Gothenburg, Sweden
- 3Regional Cancer Center West, Region Västra Götaland, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 4Department of Oncology, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 5Department Cardiology, Sahlgrenska University Hospital, Gothenburg, Sweden
- 6Department of Molecular and Clinical Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 7Department of Internal Medicine/Respiratory Medicine and Allergology, Sahlgrenska University Hospital, Gothenburg, Sweden
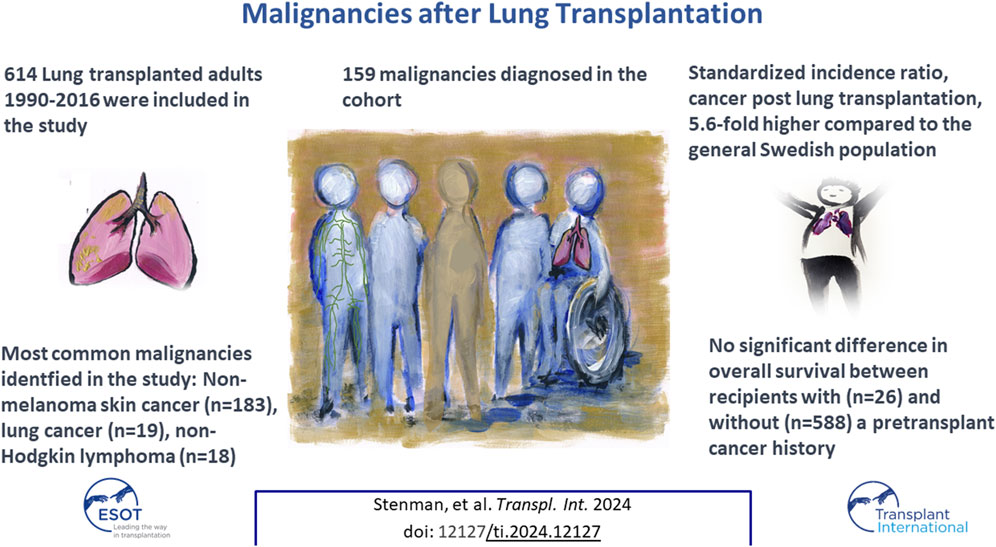
Lung transplantation (LTx) is a well-known treatment for end-stage lung disease. This study aimed to report the incidence of cancer after LTx and long-term outcome among lung transplant recipients with a pretransplant diagnosis of cancer. Patients who underwent LTx between 1990–2016 were included in the study. Detection of cancer was obtained by cross-checking the study population with the Swedish Cancer Registry and the Cause-of-Death registry. A total of 614 patients were followed for a median of 5.1 years. In all, 159 malignancies were diagnosed. The excess risk of cancer or standardized incidence ratio (SIR) following LTx was 5.6-fold compared to the general Swedish population. The most common malignancies were non-melanoma skin cancer (NMSC) (SIR 76.5 (95%CI 61.7–94.8); non-Hodgkin lymphoma (SIR 23.5, 95%CI 14.8–37.2); and lung cancer (SIR 8.89, 95%CI 5.67–13.9). There was no significant difference in overall survival between those with and without a history of cancer before LTx (p = 0.56). In total, 159 malignancies were identified after LTx, which was a 5.6-fold higher relative to the general population. A history of previous cancer yields similar survival in selected recipients, compared to those without cancer prior to LTx.
GRAPHICAL ABSTRACT |
Introduction
Lung transplantation (LTx) is nowadays an established treatment for patients with end-stage respiratory disease [1]. The immunosuppression is a crucial component to prevent graft rejection after LTx. However, there is a well-known risk of developing cancer in immunosuppressed transplant recipients [2, 3] above all thoracic transplants [4]. After solid organ transplantation, the risk has been reported to increase 2-4-fold compared with the general population [5, 6]. Lung cancer has been reported to be the most common malignancy, excluding non-melanoma skin cancer (NMSC), after LTx [7]. There are several factors associated with the increased risk of developing cancer after LTx, such as: higher age of both donor and recipient; type of immunosuppression; and type of LTx (single or bilateral) [8, 9] but also likely the fact that the 5-year survival rate after LTx has increased from 46% in 1990 to 57% in 2015 [10, 11].
Our study aims to report the incidence and long-term outcome of malignancies after LTx, and to report the outcome in those treated for cancer before LTx.
Materials and Methods
From February 1990 to December 2016, 685 LTx were performed in 633 patients at Sahlgrenska University Hospital (SUH) in Gothenburg, Sweden. We used the local patient registry at the Transplant Institute to identify those patients. We excluded those who were not Swedish citizens, and thus did not receive follow-up in Sweden after LTx (n = 19), and those who underwent re-transplantation (n = 52). The remaining 614 patients [266 (43%) men, 348 (57%) women, mean age of 50.0 years] had a median follow-up time of 5.1 years and were included in the study. Baseline characteristics for the cohort are shown in Table 1, also stratified for time era. Chronic obstructive pulmonary disease (177, 29%), pulmonary fibrosis (139, 23%), alfa-1-deficiency (104, 17%) and vascular disease (69, 11%) were the leading indications for lung transplantation in this cohort (Figure 1).
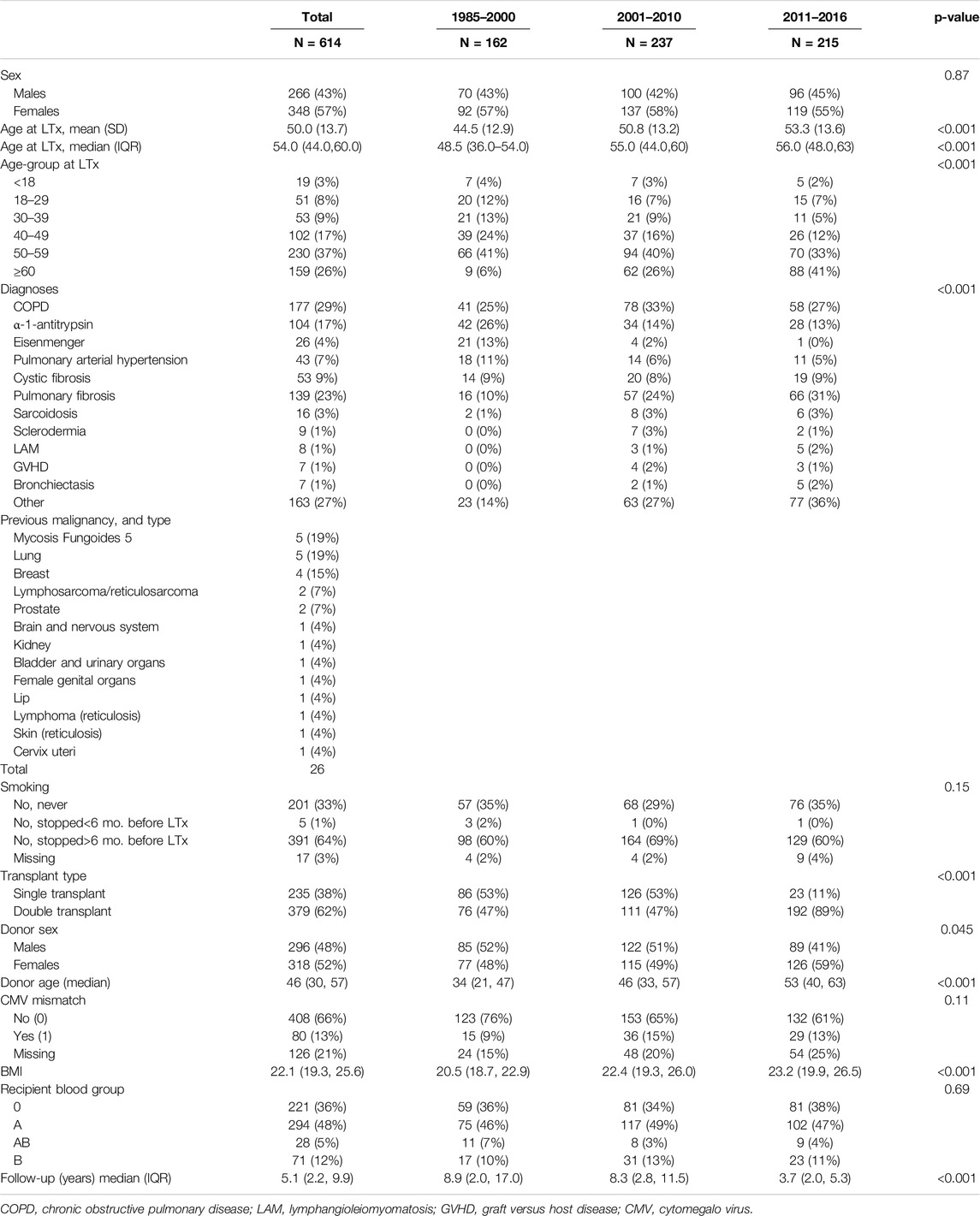
Table 1. Patient characteristics.
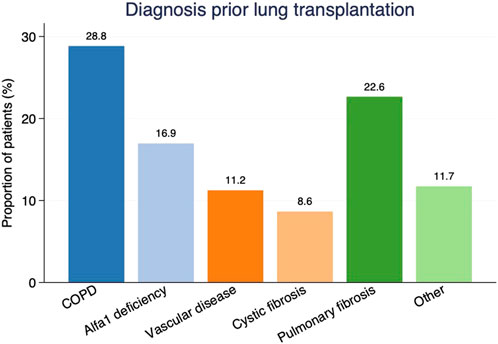
Figure 1. Etiology of lung failure as proportions of patients by diagnosis prior to lung transplantation. COPD, Chronic obstructive pulmonary disease.
Digital and scanned medical records from the transplantation unit were reviewed for all the patients. The Swedish Population Registry, which contains complete data about population changes, such as the number of births, deaths, immigration, and emigration, was used. The cancer diagnoses were obtained from the Swedish Cancer Registry (SCR) of the National Board of Health and Welfare, which contains data on all cancers diagnosed among the Swedish population since 1958. Since the start of the registry, it has been mandatory for pathologists and clinicians in Sweden to report cancer diagnosis to the SCR. Therefore, the registry has a very high coverage rate, and all our patients were crosschecked with the SCR [12] and the national Swedish cause-of-death registry to identify all patient’s survival and specifically those with a diagnosis of cancer after LTx. We did not investigate whether the patients have had basal cell carcinoma (BCC), since it is not reported in the SCR, but also since the BCC carcinoma type tends to grow slowly and metastases rarely occur [13].
At our centre, cancer, in general, has been a contraindication for listing for LTx with a few exceptions (n = 26) outlined in Table 1. We have followed International Society for Heart and Lung Transplantation (ISHLT) recommendations, and those with a cancer-free interval of at least 5 years, have been eligible for waitlisting [14]. All of the cancer diagnoses were histopathologically verified. The International Statistical Classification of Diseases (ICD-10) code was used to classify cancers. Our study was conducted in accordance with the Declaration of Helsinki and was approved by the Regional Ethical Review Board at University of Gothenburg (EPN no. 019-09, approval date 22nd Oct 2009, amendments approved 29th Nov 2010, 10th Dec 2012, 17th Dec 2013, 10th May 2017).
The immunosuppressive agents were administered according to a local protocol and has remained relatively unchanged over time. Most of the patients that underwent transplantation at SUH were treated with induction therapy (n = 599) using a t-cell antibody to minimize the risk of early acute rejection [15]. In general, all patients then received a triple combination of a calcineurin inhibitor (tacrolimus or cyclosporine), an antiproliferative agent, (mycophenolate mofetil (MMF) or Azathioprine), and steroids (Prednisone) [16]. The most used calcineurin inhibitor has been cyclosporine, and Azathioprine was replaced as the antiproliferative agent by MMF in 2004-2005.
Data are presented as means and standard deviations, medians and interquartile ranges, or numbers and percentages. Overall survival curves were generated using Kaplan-Meier estimates and comparisons between groups were performed with the log rank test. Relative survival was calculated using the Ederer II method [17]. Mortality data for the general population in Sweden was used to estimate expected survival rates. The mortality data comprised the probability of death for single-year age groups in 1-year calendar period. Cumulative incidence of cancer was analyzed using competing risk methods with death as a competing event [18]. When analyzing cancer incidence for different cancer types, person-years were calculated from date of the transplantation to the first of the following events: diagnosis of the cancer site; death; or end of surveillance period, i.e., 31 December 2018. The standardized incidence ratio (SIR) was defined as the observed number of cancers during the observation time divided by the expected number of cases, using incidence rates from the Swedish population stratified for 5-year age groups (0–4, 5–9, … 80–84, 85-), sex and calendar year. Incidence rates for different cancer sites were used from the NORDCAN project. Furthermore, the coding of cancer followed definitions according to international rules for multiple primary cancers [19]. Univariable and multivariable risk factor analyses were performed by Cox proportional hazards regression model for the development of posttransplant malignancy. The following parameters were tested by univariable analyses: age (per 10 years), sex, body mass index (BMI, <20; 20–30; >30), smoking (never; cessation >6 months before LTx listing; cessation <6 months before LTx listing), diagnostic groups, donor age (per 10 years), donor cytomegalo virus (CMV) +/−, recipient CMV+/−, CMV mismatch and recipient blood group. Significant risk factors identified in the univariate models were tested also in a multivariable model. All statistical tests were two-sided, and a p-value of <0.05 was considered statistically significant. Statistical analyses were carried out with Stata/IC 16.1.
Results
Mortality for the whole patient cohort within 30 days and 1-year post-transplant was 36/614 (6%) and 107/614 (17%), respectively. Overall survival for the whole cohort at 1, 5, and 10 years was: 82% (95%CI 79%–85%); 61% (95%CI 57%–65%); and 43% (95%CI 38%–47%), respectively. Five-year overall survival for those who underwent LTx: was 59% (95%CI: 51%–66%) between 1990 and 2000; 65% (95%CI: 59%–71%) between 2001 and 2010; and 57% (95%CI: 49%–64%) between 2011 and 2016 (Figures 2A–D). There was no significant difference in overall survival over time (p = 0.52). However, risk profile has dramatically changed over time, as illustrated by recipients above 60 years of age were only 6% in the first compared to 41% in the last time-era (p < 0.001) (Table 1).
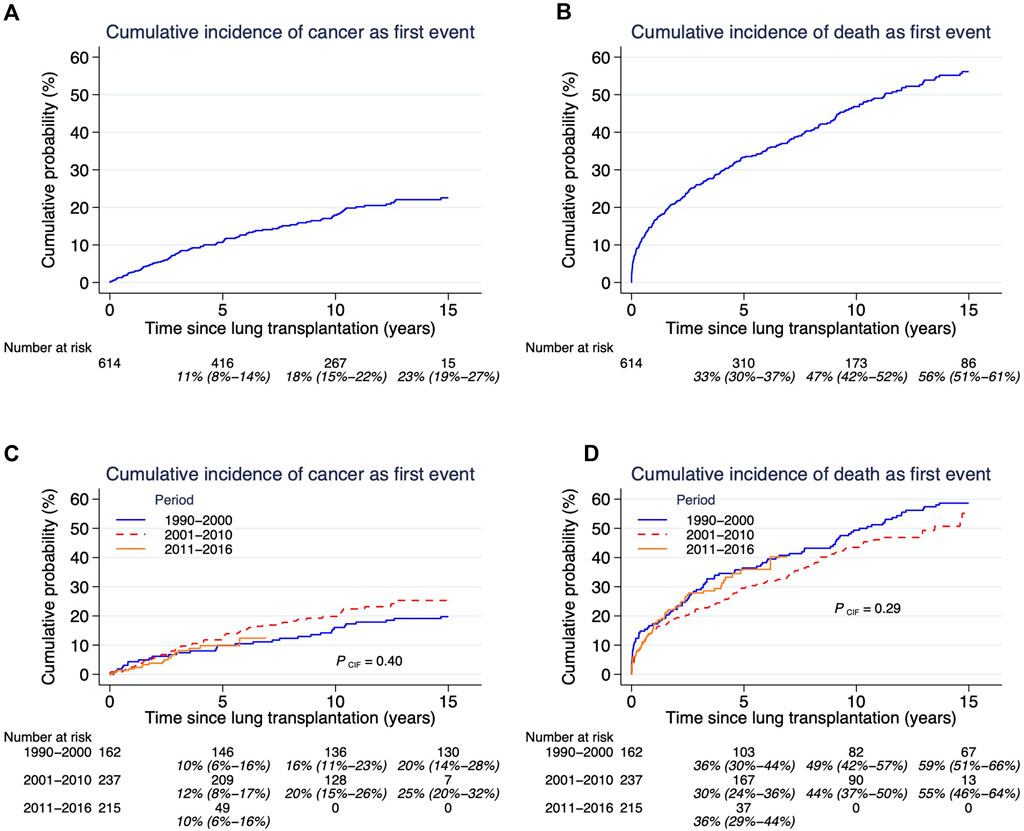
Figure 2. (A–D) Cumulative probability of cancer and cumulative incidence of death. Cumulative incidence of competing risks cancer (panel (A)] and death [panel (B)], and related to time-era after lung transplantation. Both outcomes cancer and death need to be assessed together since they are competing outcomes. Estimates and 95% confidence intervals are shown under the number of patients at risk.
A total of 159 de novo cancers were diagnosed in 111 LTx patients (48 men and 63 women) during follow-up, which corresponds to 18% of the total study population (Table 2). In comparison, 28.6 cancers would have been detected in a cohort from the general population matched by age, sex, and time period. The resulting SIR was 5.56 (95%CI 4.76–6.50) for all cancers after LTx, and 2.76 (95%CI: 2.21–3.46) after excluding NMSC.
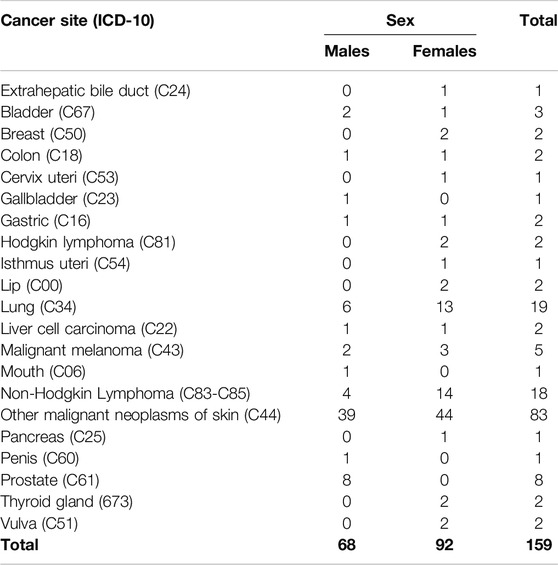
Table 2. Cancer following LTx 1990–2016.
Our study’s cumulative incidence of death was 16.4% at 1 year, 33.3% at 5 years, 46.8% at 10 years and 56.1% at 15 years post-transplantation. Corresponding numbers for the cumulative incidence of cancer were: 2.7% at 1 year; 10.6% at 5 years; 17.9% at 10 years; 22.5% at 15 years; and 23.6% at 20 years (Figures 2A, B). The cumulative incidence of de novo malignancy after LTx showed no significant difference between time eras (p = 0.40) (Figure 2C). There was no significant difference in overall mortality (p = 0.29) between the three time periods (Figure 2D).
The type and frequency of solid tumors for the total group, and shown separately for men and women, are listed in Table 2. The most common type of cancer after LTx was non-melanoma skin cancer (NMSC) (52.2% of all cancers), lung cancer (11.9% of all cancers), and non-Hodgkin Lymphoma (11.3% of all cancers). Of those 19 lung cancers that we found after LTx, the majority (n = 13) were developed in the transplanted lung, four in the native lung and two were unknown.
The SIR for cancer types diagnosed in 4 or more individuals are shown in Table 3. The excess risk of all cancers for the total population was 5.6 and similar between men and women (SIR 4.90 and SIR 6.17, respectively).
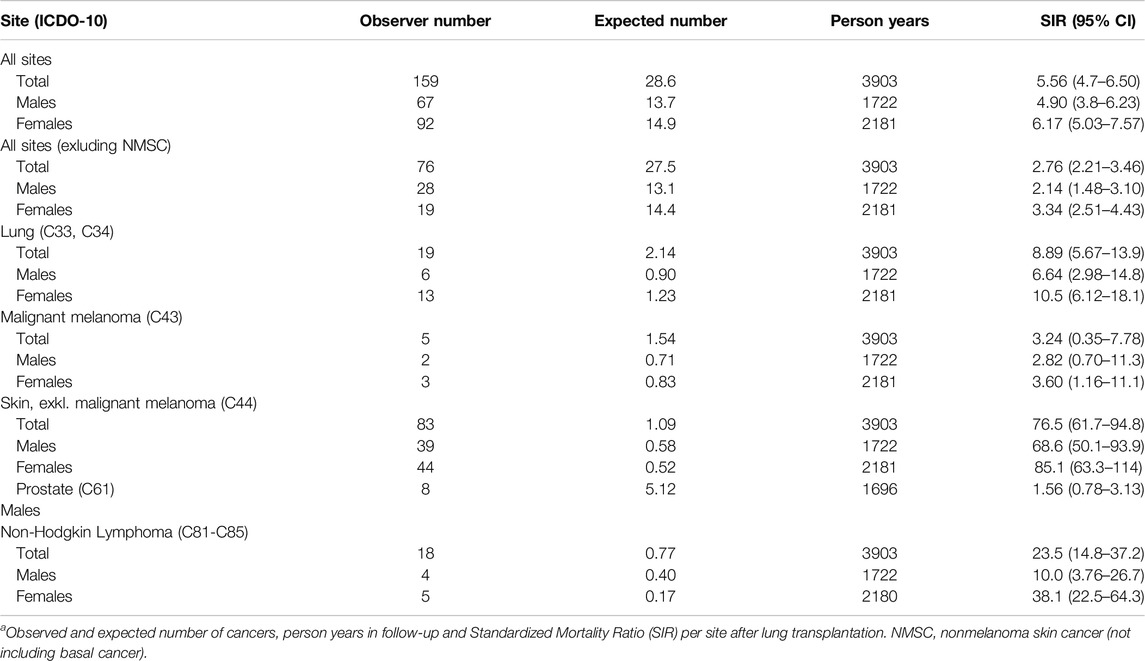
Table 3. Observed and expected cancer risks following LTxa.
The overall incidences of cancers in the cohort were higher than expected for: NMSC SIR 76.5 (95%CI 61.7–94.8); non-Hodgkin Lymphoma (SIR 23.5, 95%CI 14.8–37.2); lung cancer (SIR 8.89, 95%CI 5.67–13.9); and malignant melanoma (SIR 3.24, 95%CI 0.35–7.78).
Univariable and multivariable analysis between baseline characteristics and NMSC only is shown in Table 4. Significant risk factors in the multivariable model predicting NMSC only were: age per 10 years [HR 2.23, (95%CI 1.51–3.42), p < 0.001] and recipient blood group A [HR 2.36, (95%CI 1.01–5.53), p < 0.001].
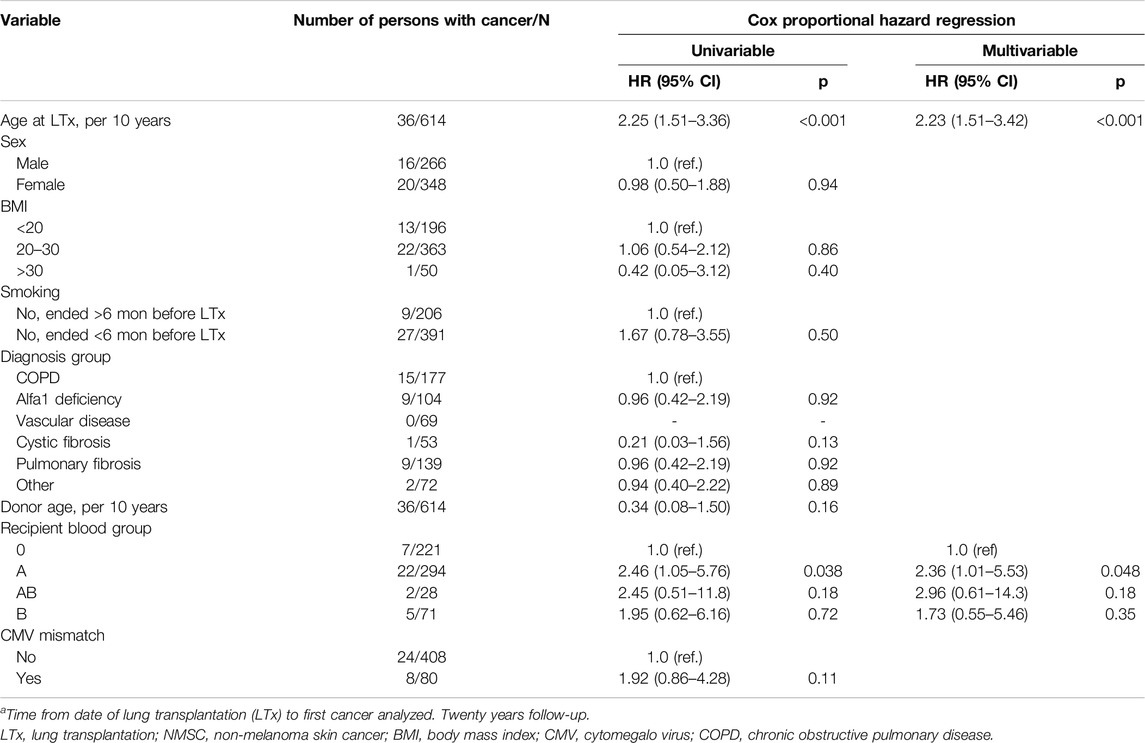
Table 4. Uni- and multivariable Cox proportional hazard regression for developing NMSC after LTxa.
We found 26 (4%) malignancies in 26 patients that had occurred 9.1 years (IQR 2.3–18.3) before LTx. Three of these were actually lung cancers detected at LTx. The median age at their first tumor before LTx was 42 years (IQR 33–53 years), and at LTx the recipient median age was 53 years (IQR 44–59). The most common cancers were: lung, breast, prostate, lymphosarcoma and reticulosarcoma which are shown in Table 1. There was no significant difference in overall survival between those with and without a history of cancer before LTx (p = 0.80) (Figure 3). Furthermore, there was no significant difference (p = 0.73) in post-LTx relative survival between cancer-free patients versus those who had experienced cancer before LTx (Figure 4).
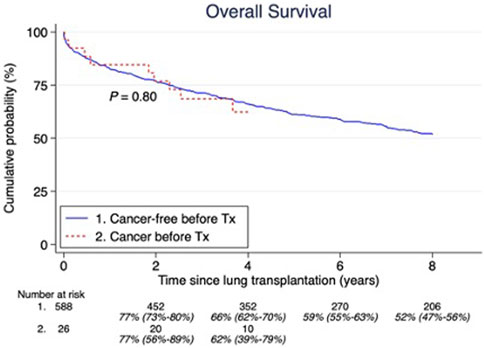
Figure 3. Pretransplant malignancy overall survival compared to those without. Estimates and 95% confidence intervals are shown under the number of patients at risk.
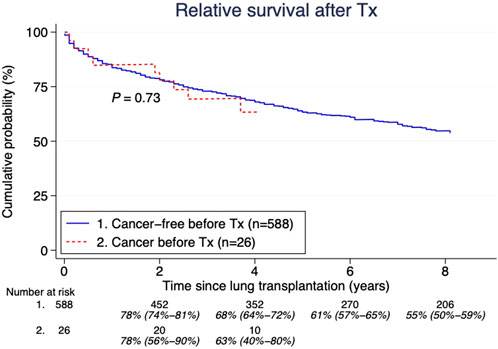
Figure 4. Pretransplant malignancy relative survival compared to those without. Estimates and 95% confidence intervals are shown under the number of patients at risk.
We have no data regarding recurrence of cancers in patients who had malignancy before LTx.
Discussion
This Swedish cohort of lung transplanted patients was studied through national obligatory cancer and cause of death registries, and we observed an overall 5.6-fold excess risk of cancer relative to the general population after a median of 5.1 years of follow-up. The majority of these cancers were NMSC, and when we excluded them from analysis, the risk relative to the general population was reduced to a 2.8-fold excess risk of developing cancer. We also noted, that there was no significantly different survival in patients who had a cancer before LTx, compared to those without a cancer.
Transplanted patients have a higher risk of developing skin cancer. It is also known that those tumors are more aggressive compared to immunocompetent patients [20]. We identified NMSC as the most common cancer, with 83 cancers in a total cohort of 614 patients (13.5%) after LTx. Rashtag et al. identified skin tumors in approximately 28% (47/166 patients) after a median follow-up of 3 years. Berastegui et al. found 39 cases of NMSC in their cohort of 1100 patients (3.5%) after a follow-up of 3 years. However, the data from these studies were not obtained from a national population registry or cancer registry, as in our study, but from individual hospital databases, which might result in missing cancer diagnoses during follow-up. In our study, among NMSC only, age and blood group were identified as independent predictors of developing NMSC after LTx. In concordance Rashtak et al. reported that age per 10 years [HR 1.54 (95%CI 1.14–2.09), p = 0.005] but also male sex [HR 2.79 (95%CI 1.48–5.28), p = 0.002] and a history of NMSC [HR 4.23 (95%CI 1.93–9.26), p =<0.001] were associated with the development of NMSC after lung transplantation [21].
In our study, when we excluded NMSC, the excess risk was 2.8 -fold to develop cancer in relation to the general population. In comparison, a large American study by Magruder et al. observed a 3.26-fold excess risk to develop cancer. In a Spanish study with 1353 patients by Berastegui et al. 125 (9.2%) developed cancer after a mean of 3.7 years, which resulted in a 5-fold higher risk compared to the general population [22]. The cumulative incidence of a de novo malignancy between 1 and 5 years after LTx was 7.9%. The most common cancer was NMSC, followed by non-Hodgkin Lymphoma and lung cancer, very similar to our observations. There were no independent predictors of cancer (excluding NMSC) in our study. Predictors of de novo malignancies following LTx presented by Magruder et al. were age, male sex and single-lung transplantation. The cumulative incidence of death was in our study 16.4% at 1 year 33.3% at 5 years, 46.8% at 10 years and 56.1% at 15 years post transplantation. Although some report limited survival among lung transplant recipients, Rashtak et al. reported a 53% mortality at 5 years and 86% at 10 years post-LTx. Our survival was better, but clearly lower than for other organ transplants [21]. Corresponding numbers, in a study with over 4000 patients, 5 years and 10 years after liver transplantation was 21% and 33% respectively [23]. A study on kidney transplantation showed a 11% mortality at 5 years and 22% after 10 years. [24]. Obviously, death as an event is a competing outcome to developing cancer, and particularly in LTx with a relatively high cumulative early death rate, the assessment of survival and cancer incidence needs to be analyzed together. Clearly, our study also shows that there was no difference in cumulative incidence of cancer between time eras, and considering that recipients have become older and sicker when accepted for LTx, this might even imply a better screening and detection of cancer in modern era.
After NMSC, non-Hodgkin lymphoma had the highest incidence (SIR 23) of cancer after LTx. A well-known complication after lung transplantation is post-transplant lympho-proliferative disease (PTLD) [25], however this entity does not have its own ICD number, and we account them as non-Hodgkin lymphoma since they are registered in that way by the SCR. In a study by Zaffiri et al. using ISHLT database with more than 19,000 lung transplant procedures registered they were able to identify 454 PTLD, resulting in a cumulative incidence of about 1% during the first year [26]. However, data from this registry was from an international community with a high risk of missing data and not compared to population in general, but our data indicate similar figures, although we cannot discriminate between PTLD and non-Hodgkin lymphomas.
We found a total of 19 lung cancers in 19 patients (3.1%), resulting in a 8.9-fold increased risk after LTx. Corroborating our findings, a French study by Chatron et al. found a total of 19 lung cancers in 463 patients after LTx (4.10%) after a median follow-up time of 21.5 months. [27]. Out of 633 lung transplant patients Pérez-Callejo et al. found that lung cancer was detected in 23 of them (3.63%), with a median follow-time of 3.5 years. [28]. Magruder et al. found the most common cancer after LTx was lung cancer (26.2% of all malignancies, SIR 6.49, 95% CI: 5.04–8.45) after a median follow-up time of 2.97 years. In a large study from the United States, Engels et al. also found an increased risk of developing lung cancer after LTx, resulting in a SIR not very different from ours SIR6.13 (95% CI, 5.18–7.21) [29]. The ISHLT reported that cancer was the 2nd most common cause of death in patients who underwent LTx five to 10 years out from transplant (17.3%) and for patients who were more than 10-year after the procedure (17.9%) [11]. In our cohort, 65% of the patients confirmed a smoking history. Earlier studies have reported that smoking history and older age have been shown to increase the risk of lung cancer after LTx, which are the same risk factors as for the general population. Interestingly, previous smoking was not identified in our study as a predictor of cancer, neither by univariable nor by multivariable testing. Those patients who received a single lung have been reported to be at a higher risk for lung cancer (compared to those who underwent double lung transplantation). The native lung left behind has with inherent risk from the underlying disease, been claimed as a possible explanation [7, 28–32]. Predictors of de novo malignancies following LTx presented by Magruder et al. were age, male sex, and single-lung transplantation [7].
Conclusion
In total 159 malignancies were identified after LTx, which was a 5.6-fold higher relative to the general population. A history of previous cancer yields similar survival in selected recipients, compared to those without cancer prior to LTx.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics Statement
Our study was conducted in accordance with the Declaration 79 of Helsinki and was approved by the Regional Ethical Review Board at University of Gothenburg (EPN no. 019-09, approval date 22nd Oct 2009, amendments approved 29th 80 Nov 2010, 10th Dec 2012, 17th Dec 2013, 10 81th May 2017).
Author Contributions
CS: conceived and designed the analysis, collected the data, wrote the paper. AW: conceived and designed the analysis. EH: collected the data, performed the analysis, wrote the paper. KK: conceived and designed the analysis, collected the data, wrote the paper. JM: collected the data, wrote the paper. GD: conceived and designed the analysis, collected the data, performed the analysis, wrote the paper. All authors contributed to the article and approved the submitted version.
Funding
The author(s) declare(s) that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The aim of this article is to investigate cancer after lung transplantation. My colleagues and I published a paper entitled “Sun protection behaviour in organ transplant recipients and non-transplant patients attending a dermatology outpatient clinic in Sweden: A questionnaire survey.” Photodermatol Photoimmunol Photomed. 2022 Mar; 38(2):132-140. doi: 10.1111/phpp.12726. Epub 2021 Aug 30.PMID: 34416022 This article included a survey among 696 organ transplant recipients (lung, heart, kidney, liver, and pancreas) focused on sun habits after transplantation.
Abbreviations
BCC, basal cell carcinoma; BMI, body mass index; CI, confidence interval; CMV, cytomegalo virus; COPD, chronic obstructive pulmonary disease; GVHD, graft versus host disease, HR, hazard ratio; ICD, International Statistical Classification of Diseases; ISHLT, International Society for Heart and Lung Transplantation; LAM, lymphangioleiomyomatosis; LTx, lung transplantation; NMSC, non-melanoma skin cancer; MMF, mycophenolate mofetil; PTLD, post-transplant lympho-proliferative disease; SCR, Swedish cancer registry; SIR, standardized incidence ratio; SUH, Sahlgrenska University Hospital.
References
1. Yusen, RD, Edwards, LB, Dipchand, AI, Goldfarb, SB, Kucheryavaya, AY, Levvey, BJ, et al. The Registry of the International Society for Heart and LUNG Transplantation: Thirty-Third Adult LUNG and Heart-Lung Transplant Report-2016; Focus Theme: Primary Diagnostic Indications for Transplant. J Heart Lung Transpl (2016) 35(10):1170–84. doi:10.1016/j.healun.2016.09.001
2. Adami, J, Gabel, H, Lindelof, B, Ekström, K, Rydh, B, Glimelius, B, et al. Cancer RISK Following Organ Transplantation: A Nationwide Cohort Study in Sweden. Br J Cancer (2003) 89(7):1221–7. doi:10.1038/sj.bjc.6601219
3. Hall, EC, Pfeiffer, RM, Segev, DL, and Engels, EA. Cumulative Incidence of Cancer After Solid Organ Transplantation. Cancer (2013) 119(12):2300–8. doi:10.1002/cncr.28043
4. Krynitz, B, Edgren, G, Lindelof, B, Baecklund, E, Brattström, C, Wilczek, H, et al. RISK of SKIN Cancer and Other Malignancies in Kidney, Liver, Heart and LUNG Transplant Recipients 1970 to 2008--a Swedish Population-Based Study. Int J Cancer (2013) 132(6):1429–38. doi:10.1002/ijc.27765
5. Collett, D, Mumford, L, Banner, NR, Neuberger, J, and Watson, C. Comparison of the Incidence of Malignancy in Recipients of Different Types of Organ: A UK Registry Audit. Am J Transplant : official J Am Soc Transplant Am Soc Transpl Surgeons (2010) 10(8):1889–96. doi:10.1111/j.1600-6143.2010.03181.x
6. Ippoliti, G, Rinaldi, M, Pellegrini, C, and Vigano, M. Incidence of Cancer After Immunosuppressive Treatment for Heart Transplantation. Crit Rev Oncol Hematol (2005) 56(1):101–13. doi:10.1016/j.critrevonc.2005.03.013
7. Magruder, JT, Crawford, TC, Grimm, JC, Kim, B, Shah, AS, Bush, EL, et al. RISK Factors for De NOVO Malignancy Following LUNG Transplantation. Am J Transpl (2017) 17(1):227–38. doi:10.1111/ajt.13925
8. Dickson, RP, Davis, RD, Rea, JB, and Palmer, SM. HIGH Frequency of Bronchogenic Carcinoma After Single-Lung Transplantation. J Heart Lung Transpl (2006) 25(11):1297–301. doi:10.1016/j.healun.2006.09.009
9. Opelz, G, and Dohler, B. Lymphomas After Solid Organ Transplantation: A Collaborative Transplant Study Report. Am J Transplant : official J Am Soc Transplant Am Soc Transpl Surgeons (2004) 4(2):222–30. doi:10.1046/j.1600-6143.2003.00325.x
10. Yusen, RD, Edwards, LB, Kucheryavaya, AY, Benden, C, Dipchand, AI, Goldfarb, SB, et al. The Registry of the International Society for Heart and LUNG Transplantation: Thirty-Second Official Adult LUNG and Heart-Lung Transplantation Report--2015; Focus Theme: Early Graft Failure. J Heart Lung Transpl (2015) 34(10):1264–77. doi:10.1016/j.healun.2015.08.014
11. Chambers, DC, Yusen, RD, Cherikh, WS, Goldfarb, SB, Kucheryavaya, AY, Khusch, K, et al. The Registry of the International Society for Heart and LUNG Transplantation: Thirty-Fourth Adult LUNG and Heart-Lung Transplantation Report-2017; Focus Theme: Allograft Ischemic TIME. J Heart Lung Transpl (2017) 36(10):1047–59. doi:10.1016/j.healun.2017.07.016
12. Barlow, L, Westergren, K, Holmberg, L, and Talbäck, M. The Completeness of the Swedish Cancer Register: A Sample Survey for YEAR 1998. Acta Oncol (2009) 48(1):27–33. doi:10.1080/02841860802247664
13. Rubin, AI, Chen, EH, and Ratner, D. Basal-Cell Carcinoma. N Engl J Med (2005) 353(21):2262–9. doi:10.1056/NEJMra044151
14. Weill, D, Benden, C, Corris, PA, Dark, JH, Davis, RD, Keshavjee, S, et al. A Consensus Document for the Selection of LUNG Transplant Candidates: 2014—An Update FROM the Pulmonary Transplantation Council of the International Society for Heart and LUNG Transplantation. The J Heart Lung Transplant (2015) 34(1):1–15. doi:10.1016/j.healun.2014.06.014
15. Van den Hoogen, MW, Hoitsma, AJ, and Hilbrands, LB. Anti-T-cell Antibodies for the Treatment of Acute Rejection After Renal Transplantation. Expert Opin Biol Ther (2012) 12(8):1031–42. doi:10.1517/14712598.2012.689278
16. Gilljam, M, Nystrom, U, Dellgren, G, Skog, I, and Hansson, L. Survival After LUNG Transplantation for Cystic Fibrosis in Sweden. Eur J Cardiothorac Surg (2017) 51(3):571–6. doi:10.1093/ejcts/ezw328
17. Ederer, F, Axtell, LM, and Cutler, SJ. The Relative Survival RATE: A Statistical Methodology, Natl Cancer Inst Monogr (1961) 6:101–21.
18. Fine, JP, and Gray, RJ. A Proportional Hazards Model For the Subdistribution of A Competing RISK. J Am Stat Assoc (1999) 94(446):496–509. doi:10.1080/01621459.1999.10474144
19. International rules for multiple primary cancers (ICD-0 third edition). International Rules for Multiple Primary Cancers (ICD-0 Third Edition). Eur J Cancer Prev: official J Eur Cancer Prev Organisation (Ecp) (2005) 14(4):307–8. doi:10.1097/00008469-200508000-00002
20. Euvrard, S, Kanitakis, J, Pouteil-Noble, C, Disant, F, Dureau, G, Finaz de Villaine, J, et al. Aggressive Squamous CELL Carcinomas in Organ Transplant Recipients. Transplant Proc (1995) 27(2):1767–8.
21. Rashtak, S, Dierkhising, RA, Kremers, WK, Peters, SG, Cassivi, SD, and Otley, CC. Incidence and RISK Factors For SKIN Cancer Following LUNG Transplantation. J Am Acad Dermatol (2015) 72(1):92–8. doi:10.1016/j.jaad.2014.09.010
22. Berastegui, C, LaPorta, R, López-Meseguer, M, Romero, L, Gómez-Ollés, S, Riera, J, et al. Epidemiology and RISK Factors For Cancer After LUNG Transplantation. Transpl Proc (2017) 49(10):2285–91. doi:10.1016/j.transproceed.2017.09.043
23. Jain, A, Reyes, J, Kashyap, R, Dodson, SF, Demetris, AJ, Ruppert, K, et al. Long-Term Survival After Liver Transplantation in 4,000 Consecutive Patients At A Single Center. Ann Surg (2000) 232(4):490–500. doi:10.1097/00000658-200010000-00004
24. Scheffner, I, Gietzelt, M, Abeling, T, Marschollek, M, and Gwinner, W. Patient Survival After Kidney Transplantation: Important Role of Graft-Sustaining Factors as Determined By Predictive Modeling Using Random Survival Forest Analysis. Transplantation (2020) 104(5):1095–107. doi:10.1097/TP.0000000000002922
25. Penn, I, Hammond, W, Brettschneider, L, and Starzl, TE. Malignant Lymphomas in Transplantation Patients. Transpl Proc (1969) 1(1):106–12.
26. Zaffiri, L, Long, A, Neely, ML, Cherikh, WS, Chambers, DC, and Snyder, LD. Incidence and Outcome of Post-transplant Lymphoproliferative Disorders in Lung Transplant Patients: Analysis of ISHLT Registry. J Heart Lung Transpl (2020) 39(10):1089–99. doi:10.1016/j.healun.2020.06.010
27. Chatron, E, Dégot, T, Salvaterra, E, Dumazet, A, Porzio, M, Hirschi, S, et al. Lung Cancer After LUNG Transplantation: An Analysis of 25 Years of Experience in a Single Institution. Clin Transplant (2019) 33(1):e13446. doi:10.1111/ctr.13446
28. Pérez-Callejo, D, Torrente, M, Parejo, C, Laporta, R, Ussetti, P, and Provencio, M. Lung Cancer in LUNG Transplantation: Incidence and Outcome. Postgrad Med J (2018) 94(1107):15–9. doi:10.1136/postgradmedj-2017-134868
29. Engels, EA, Pfeiffer, RM, Fraumeni, JF, Kasiske, BL, Israni, AK, Snyder, JJ, et al. Spectrum of Cancer RISK Among US Solid Organ Transplant Recipients. Jama (2011) 306(17):1891–901. doi:10.1001/jama.2011.1592
30. Triplette, M, Crothers, K, Mahale, P, Yanik, EL, Valapour, M, Lynch, CF, et al. Increased RISK of LUNG Cancer in LUNG Transplant Recipients in the United States. Am J Of Respir And Crit Care Med (2017) 195.
31. Raviv, S, Hawkins, KA, DeCamp, MM, and Kalhan, R. LUNG Cancer in Chronic Obstructive Pulmonary Disease: Enhancing Surgical Options and Outcomes. Am J Respir Crit Care Med (2011) 183(9):1138–46. doi:10.1164/rccm.201008-1274CI
Keywords: cancer, immunosuppression, heart transplantation, epidemiology, cohort study
Citation: Stenman C, Wallinder A, Holmberg E, Karason K, Magnusson J and Dellgren G (2024) Malignancies After Lung Transplantation. Transpl Int 37:12127. doi: 10.3389/ti.2024.12127
Received: 26 September 2023; Accepted: 01 August 2024;
Published: 09 September 2024.
Copyright © 2024 Stenman, Wallinder, Holmberg, Karason, Magnusson and Dellgren. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Göran Dellgren, Z29yYW4uZGVsbGdyZW5AdmdyZWdpb24uc2U=, Y2Fyb2xpbmUuc3Rlbm1hbkB2Z3JlZ2lvbi5zZQ==