 Carlos Jiménez-Romero1,2†
Carlos Jiménez-Romero1,2† Iago Justo Alonso1,2*†
Iago Justo Alonso1,2*† Oscar Caso Maestro1,2
Oscar Caso Maestro1,2 Alejandro Manrique Municio1,2Álvaro García-Sesma1,2Jorge Calvo Pulido1,2Félix Cambra Molero1,2Carmelo Loinaz Segurola1,2Cristina Martín-Arriscado3Anisa Nutu1,2Alberto Marcacuzco Quinto1,2
Alejandro Manrique Municio1,2Álvaro García-Sesma1,2Jorge Calvo Pulido1,2Félix Cambra Molero1,2Carmelo Loinaz Segurola1,2Cristina Martín-Arriscado3Anisa Nutu1,2Alberto Marcacuzco Quinto1,2- 1Unit of Hepato-Pancreato-Biliary Surgery and Abdominal Organ Transplantation, Doce de Octubre University Hospital, Madrid, Spain
- 2Department of Surgery, Faculty of Medicine, Complutense University, Madrid, Spain
- 3Clinical Research Department, Instituto de Investigación (imas12), Madrid, Spain
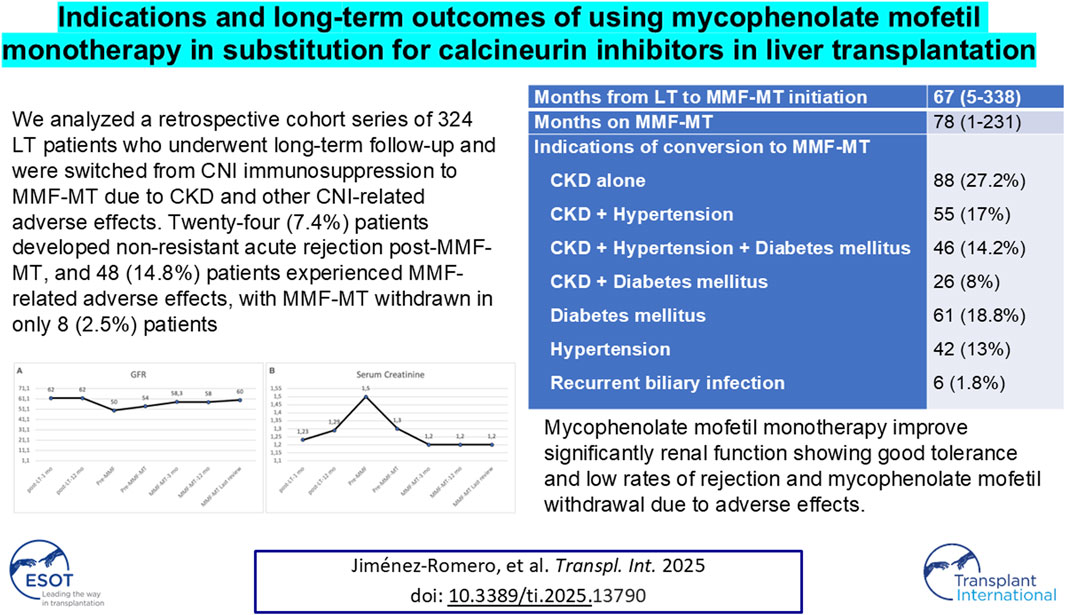
Switching the use of calcineurin inhibitors (CNIs), as basal immunosuppression in liver transplantation (LT) patients, for that of mycophenolate mofetil monotherapy (MMF-MT) is currently considered a good measure in recipients with chronic kidney disease (CKD) and other CNI-related adverse effects. We analyzed a retrospective cohort series of 324 LT patients who underwent long-term follow-up and were switched from CNI immunosuppression to MMF-MT due to CKD and other CNI-related adverse effects (diabetes, hypertension, infection). The median time on MMF-MT was 78 months. The indication for MMF-MT was CKD alone or associated with CNI-related adverse effects in 215 patients, diabetes in 61, hypertension in 42, and recurrent cholangitis in 6. Twenty-four (7.4%) patients developed non-resistant acute rejection post-MMF-MT, and 48 (14.8%) patients experienced MMF-related adverse effects, with MMF-MT withdrawn in only 8 (2.5%) patients. In the comparison between the pre-MMF-MT period and the last outpatient review, using a repeated measures model and taking each patient as its own comparator, we demonstrated a significant increase in GFR and significant decrease in creatinine and ALT values, remaining the other variables (diabetes, hypertension, and hematological and AST) within similar levels. Five-year survival post-MMF-MT conversion was 75.3%. MMF-MT significantly improved renal function, was well tolerated, and had a low rejection rate.
Introduction
Currently, calcineurin inhibitors (CNIs) are the standard therapy for maintenance immunosuppression in patients who undergo liver transplantation (LT), with a preference for tacrolimus over cyclosporine [1]. However, CNI drugs are often associated with several adverse effects, such as: nephrotoxicity, chronic kidney disease (CKD), neurotoxicity, diabetes, arterial hypertension, cardiovascular complications, hyperlipidemia, hyperuricemia, hepatocellular carcinoma (HCC) recurrence, de novo malignancies and infections [2–7]. The use of tacrolimus is associated with improved renal function than the use of CyA [4], especially when a low dose of tacrolimus is combined with mycophenolate mofetil (MMF) [8–10]. Conversely, some immunosuppressive changes have been introduced to prevent or reduce the adverse effects related to CNIs, such as the minimization or substitution of CNIs for either MMF monotherapy (MT) or the mTORi-MT regimen [11–13]. The term “immunosuppression minimization” is defined as the lowest dose of immunosuppressive drugs compatible with a rejection-free state and the absence of clinically adverse effects [14, 15].
Mycophenolic acid (MPA) is the pharmacokinetically active product of MMF with potent inhibitory effects on de novo purine synthesis and T and B lymphocyte proliferation. Nevertheless, several adverse effects have also been associated with the use of MMF, such as myelotoxicity (anemia, leukopenia, and thrombocytopenia) and gastrointestinal symptoms (diarrhea, nausea, vomiting, abdominal pain, hemorrhage) [16–19], as well as teratogenicity [20]. Despite these drawbacks, switching from CNIs to MMF-MT is currently considered a good measure to improve kidney function in patients who develop post-LT CKD [16, 18, 19, 21–24], hypertension [16, 21, 22, 25], and diabetes mellitus [17, 22]. The presence of hypertension, with a prevalence of approximately 70% in LT patients, increases the risk of chronic kidney disease (CKD) and cardiovascular disease development and is associated with a higher mortality risk more than 1 year after LT [26].
The aim of this retrospective study is to describe our experience switching CNI immunosuppression to that with MMF-MT in LT patients who develop CNI-related adverse effects throughout a long-term follow-up. To our knowledge, this study is the largest single-center study reported using MMF-MT in LT patients.
Patients and Methods
Population and Study Design
Between April 1986 and June 2022, we performed a total of 2,204 LTs at our institution. For this study, we recorded the data of 324 LT recipients among a total of 1,697 who underwent LT between January 1997 (the first patient included in MMF-MT) and June 2022 and were subsequently converted from immunosuppression with combined CNI-MT or CNI + MMF to MMF-MT. In this retrospective single-center cohort study, we analyzed the impact of MMF-MT on toxicity or adverse effects (CKD, hypertension, diabetes mellitus, and recurrent biliary infection) in patients previously undergoing immunosuppression with CNIs and the incidence of rejection and adverse effects related to the use of MMF-MT.
The inclusion criteria for conversion from CNI-MT to MMF-MT were as follows: patients >18 years usually with more than 2 years of follow-up after LT, stable liver graft function and the absence of acute rejection in the last year before MMF-MT conversion. This study was closed on December 2023, and all patients were followed for at least 1.5 years after conversion to MMF-MT. Medical history of liver retransplantation, previous renal transplant, and hepatocellular carcinoma recurrence were considered exclusionary for this study. Informed consent for MMF-MT was obtained from all patients included in this study.
This research was performed in accordance with the ethical guidelines of the 1964 Helsinki Declaration and its later amendments and was approved by our Institutional Review Board (Research Registry no 24/025). The need for local clinical research ethics committee approval was waived because of the retrospective nature of the research.
Baseline Data
The following patient data were retrospectively collected: age, sex, body mass index (BMI), Child‒Pugh and MELD scores, presence of arterial hypertension or diabetes, LT indications, pre-LT recipient laboratory values, type of donors and graft steatosis, type of CNI, rate and grade of post-LT acute rejection, median time elapsed from LT to initiation of MMF-MT and median time on MMF-MT, indications of conversion to MMF-MT, rate of post-MMF-MT acute rejection and therapy, adverse effects related to MMF-MT, causes of MMF-MT withdrawal, and the need for dialysis and kidney transplant during the follow-up of MMF-MT patients.
Determinations were taken of post-MMF-MT laboratory parameters (serum glucose, hematological, kidney and liver function values), doses of MMF and blood levels of MPA throughout the follow-up at different periods [pre-MMF-MT (combined CNI-MMF), 3, 6, and 12 months post-MMF-MT, and at the end of the study]. Comparisons between the variables (diabetes, hypertension, and hematological, kidney and liver function) of pre-MMF-MT patients and the final outpatient review of MMF-MT patients were performed. The sample was divided into two eras (first era: 1999–2011; second era: 2012–2023), that were compared regarding acute rejection, adverse effects, causes MMF-MT withdrawal and patient survival was performed between both groups of patients.
Variable Definitions
CKD was defined as a GFR <60 mL/min/1.73 m2 or markers of kidney damage, or both, of at least 3 months in duration, and estimation of the GFR was performed according to the CKD-EPI equation [27]. Arterial hypertension was defined as a systolic blood pressure >140 mmHg and/or a diastolic blood pressure >90 mmHg on three consecutive measurements within three to 6 months [28]. A diagnosis of diabetes mellitus was established if fasting plasma glucose was ≥126 mg/dL or if 2 h plasma glucose levels were ≥200 mg/dL, according to the ADA criteria [29]. Anemia was defined as hemoglobin <8 g/dL; leukopenia was defined as a white blood cell count <2,500/mm3; and thrombocytopenia was defined as a platelet count <60,000/mm3. The diagnosis of acute rejection was performed by liver graft biopsy or empirically by alteration of liver function tests. Acute rejection was classified according to the Banff grades [30].
Immunosuppression
The initial immunosuppressive regimen comprised CNI (cyclosporine or tacrolimus) and steroids with or without MMF. Steroids were discontinued between 3 and 6 months post-transplantation. The dose of tacrolimus was adjusted to achieve target blood trough levels of 10–15 ng/mL for the first month, 7–9 ng/mL within the first year, 5 ng/mL between the 2nd and 4th years, and between 4 and 5 ng/mL thereafter. The dose of oral cyclosporine was adjusted to maintain blood trough levels between 200 and 300 ng/mL for the first month and between 150 and 200 thereafter.
In the presence of severe adverse effects associated with CNIs, such as renal dysfunction, diabetes, and hypertension, MMF was introduced to reduce CNI levels by half. Conversion from CNI to MMF-MT was performed on long-term follow-up recipients with stable liver function, starting at a dose of 500 mg of MMF twice daily, which was subsequently increased up to 1 g twice daily, followed by a gradual reduction in CNI until complete withdrawal. For patients on MMF-MT, MMF was administered at a dose capable of maintaining MPA levels between 2–4 ng/mL. Currently, the period from the introduction of MMF to CNI withdrawal is between 1 and 2 months, with posterior review in the outpatient clinic at 15, 30, and 90 days and routine follow-up every 6 months thereafter.
Patients on MMF-MT who showed liver dysfunction or biopsy-proven acute rejection grade I/II were initially treated with increasing doses of MMF (up to 1 g/12 h) to achieve MPA levels between 2–4 ng/mL or with 0.5–1 g of methylprednisolone intravenously for 3 days. Tacrolimus, cyclosporine or mTORi were reintroduced in cases of resistant acute rejection. In the presence of moderate-severe adverse effects, MMF was reduced or withdrawn and CNI was reintroduced. The dose of MMF was adjusted according to the protocol based on blood levels and liver function.
Statistical Analysis
Qualitative variables are expressed as absolute numbers, and relative frequencies are expressed as percentages. Associations were analyzed via the chi-square test or Fisher’s exact test, when applicable. Most quantitative variables did not have a normal distribution according to the Kolmogorov–Smirnov test; therefore, all the quantitative variables are expressed as medians and percentiles and are expressed between 0 and 100. The relationships between quantitative variables were analyzed via the Mann–Whitney U test. A repeated measures model was used, taking each patient as its own comparator, in order to evaluate different key parameters pre and post MMF-MT. Survival analysis was performed via the Kaplan–Meier estimator and the log-rank test. A p value of <0.05 was considered to indicate statistical significance. Statistical analysis was performed via SPSS Statistics, version 25 (SPSS, Inc., Chicago, IL, United States).
Results
Recipient and Donor Characteristics
From January 1997 to June 2022, a total of 1,697 patients underwent LT and were immunosuppressed with CNI. A group of 324 patients was initially treated with CNI standard immunosuppression (252 with tacrolimus-based and 72 with cyclosporine-based). The median recipient age was 55 (19–70) years, and the median MELD score was 15 (6–35). Alcoholic cirrhosis, hepatitis C virus (HCV) cirrhosis and HCC were the most frequent indications for LT.
Concerning pre-LT laboratory variables, the median serum creatinine value was 1.1 (0.5–1.9) mg/dL, and the median GFR was 70.2 (36–111) mL/min/1.73 m2. Livers from donation after brain death (DBD) were used in 289 (89.2%) patients, and livers from donors with uncontrolled circulatory death (uDCD) were used in 16 (4.9%) patients. The remaining characteristics of the recipients and donors are detailed in Table 1.
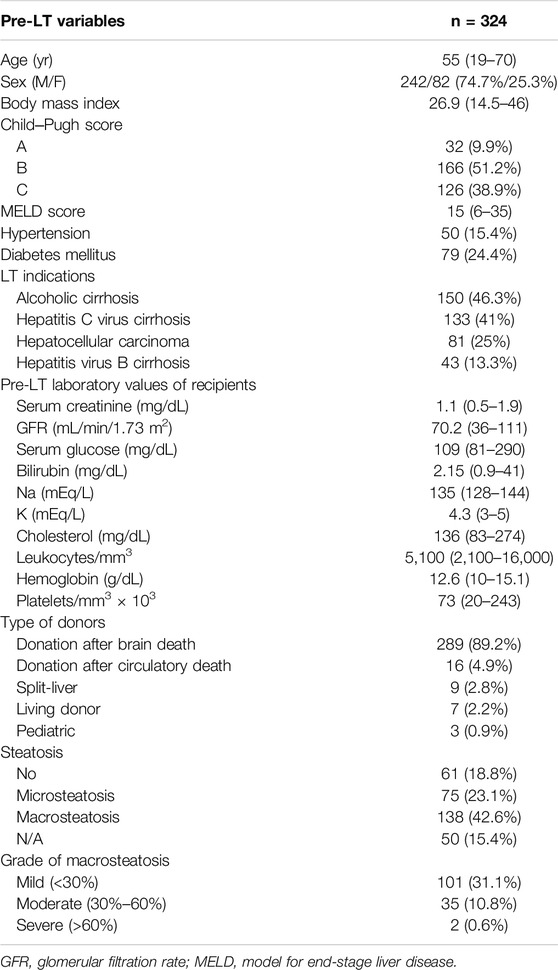
Table 1. Characteristics of recipients and donors converted from CNI to MMF-MT.
Pre- and Post-MMF-MT Characteristics
Immediately after LT, tacrolimus-based immunosuppression was used in 252 (77.8%) patients vs. the 72 (22.2%) who received cyclosporine-based immunosuppression. One episode of acute rejection after LT occurred in 90 (27.8%) patients, and two or more episodes in 23 (7.1%), with rejection grades I-II appearing in 106 (32.7%) patients.
The median time from LT to the initiation of MMF-MT was 67 (5–338) months, whereas the median time from the initiation of the combined MMF-CNI or CNI-alone regimen to CNI withdrawal and switch to MMF-MT was 18 (0–170) months. The overall median follow-up time of patients on MMF-MT was 68 (1–231) months.
The indication for switching from CNI to MMF-MT was CKD in 215 (66.4%) patients (CKD on its own in 88 patients and associated with hypertension in 55 patients, diabetes and hypertension in 46 patients, and associated with diabetes in 26 patients), diabetes mellitus on its own in 61 (18.8%) patients, hypertension in 42 (13%) patients, and recurrent biliary infection in 6 (1.8%) patients.
Just before shifting from tacrolimus to MMF-MT, 228 (70.3%) patients were on tacrolimus immunosuppression (associated with MMF in 220 patients and monotherapy in 8 patients), and 96 patients were on cyclosporine immunosuppression (associated with MMF in 91 patients and monotherapy in 5 patients).
Twenty-four (7.4%) patients experienced acute rejection after conversion from CNI to MMT-MT; 14 (4.3%) patients were diagnosed by liver biopsy (grade I/II in 13), and 10 (3.1%) were empirically diagnosed by liver dysfunction. All patients responded completely to rejection therapy (steroids and reintroduction of tacrolimus [20 patients], cyclosporine [1 patient], or mTORi [3 patients]). Forty-eight (14.8%) patients developed adverse effects related to MMF-MT, with the most common diarrhea (5.6%), vomiting (1.9%), and leukopenia (5.9%).
MMF-MT withdrawal was performed in 42 (12.9%) patients, due to de novo tumors in 13 (4%) patients (substitution of MMF-MT by mTORi monotherapy), biopsy-proven rejection in 8 (2.5%), liver dysfunction in 6 (1.8%), liver retransplantation in 4 (1.2%), kidney retransplantation in 3 (0.9%) and adverse effects in 8 (2.5%). With respect to side effects, MMF-MT withdrawal was performed in 5 (1.5%) patients with persistent chronic diarrhea despite a change from MMF to mycophenolate sodium salt and in 3 (0.8%) patients with leukopenia (Table 2). The remaining patients with adverse effects improved with a reduction in MMF dosage.
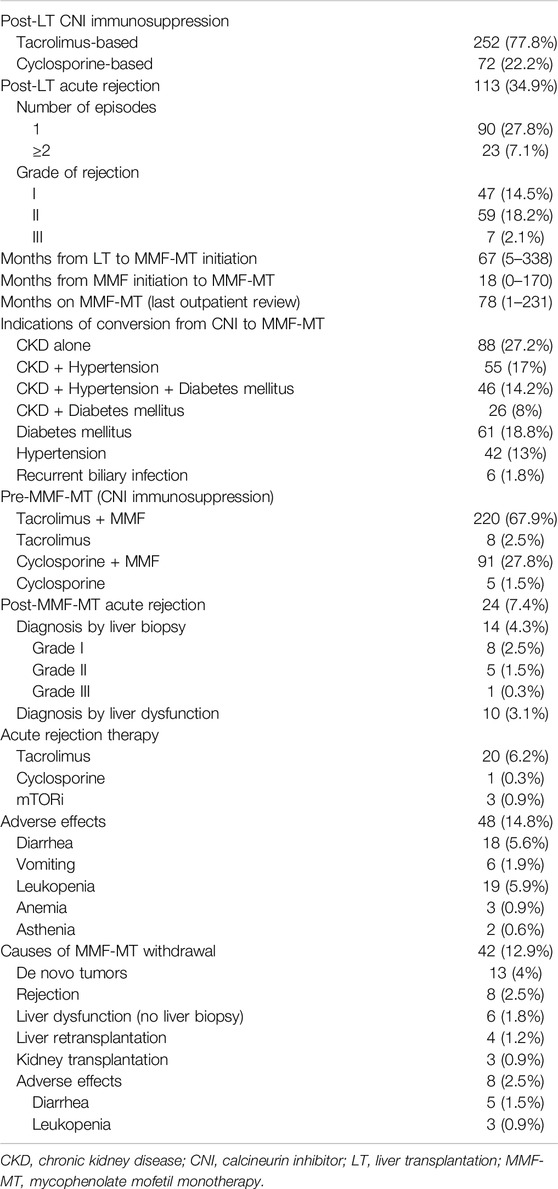
Table 2. Pre- and post-MMF-MT rejection, adverse effects and MMF withdrawal.
Dosage of MMF and Monitoring of MPA Levels Through Follow-Up
The dosage of MMF was adjusted according to MPA plasma levels, resulting in great variability among patients. The overall daily dose of MMF and median MPA plasma levels in patients on combined CNI-MMF therapy (just before conversion to MMF-MT) and in MMF-MT patients after 3, 6, and 12 months and at the last outpatient review (median period of 78 months) are detailed in Table 3, where it can be observed that MPA median plasma levels were similar in the pre-MMF-MT period or combined CNI-MMF [2.6 (0.1–15 ng/dL)] and at the last outpatient review [2.7 (0.2–15) ng/dL; p = 0.527].
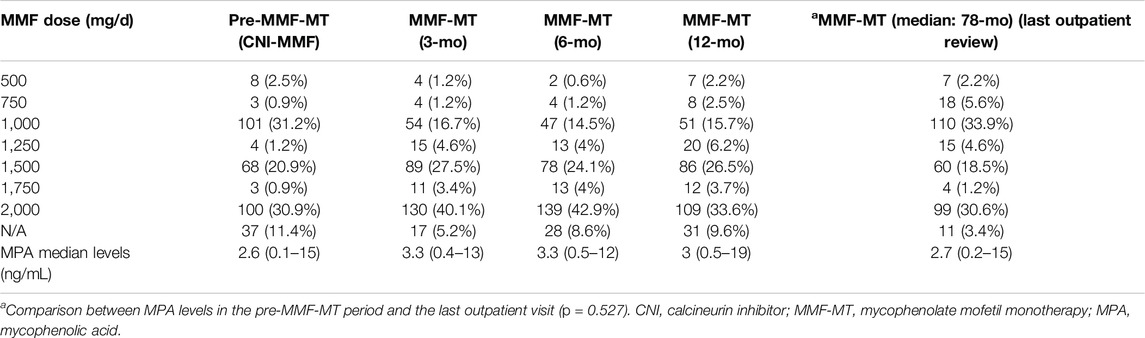
Table 3. Overall daily doses of MMF and monitoring of MPA levels during follow-up.
Comparison of Characteristics Between Pre-MMF-MT and Final Review
The frequency of diabetes and hypertension and laboratory values of hematological, renal and liver function during long-term follow-up are shown in Table 4. In the comparison of the median values of variables between the pre-MMF-MT period (combined MMF-CNI or CNI alone) and the last outpatient review on MMF-MT (median of 78 months), only the median GFR value was significantly greater in the last review on MMF-MT [56 (15–126) mL/min/1.73 m2 vs. 61 (7–134) mL/min/1.73 m2; p = 0.001], whereas the frequency of diabetes and hypertension and laboratory values of hematological variables, serum creatinine and liver function (AST and ALT) did not show significant differences between the two periods (Figures 1, 2). The 6 patients who were switched to MMF-MT due to biliary infection did not experience any new episodes of recurrent biliary cholangitis. On the other hand, using a repeated measures model, taking each patient as its own comparator, we found a statistically significant increase in GFR, statistically significant decrease in creatinine and statistically lower value of ALT at the last outpatient review in comparison with the pre-MMF-MT period (combined MMF-CNI or CNI alone) (Table 4).
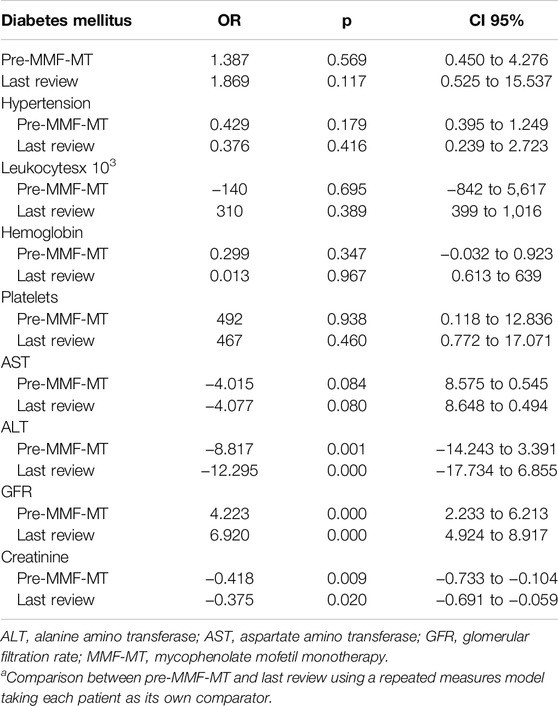
Table 4. Comparison of variables between the pre-MMF-MT period and last reviewa.
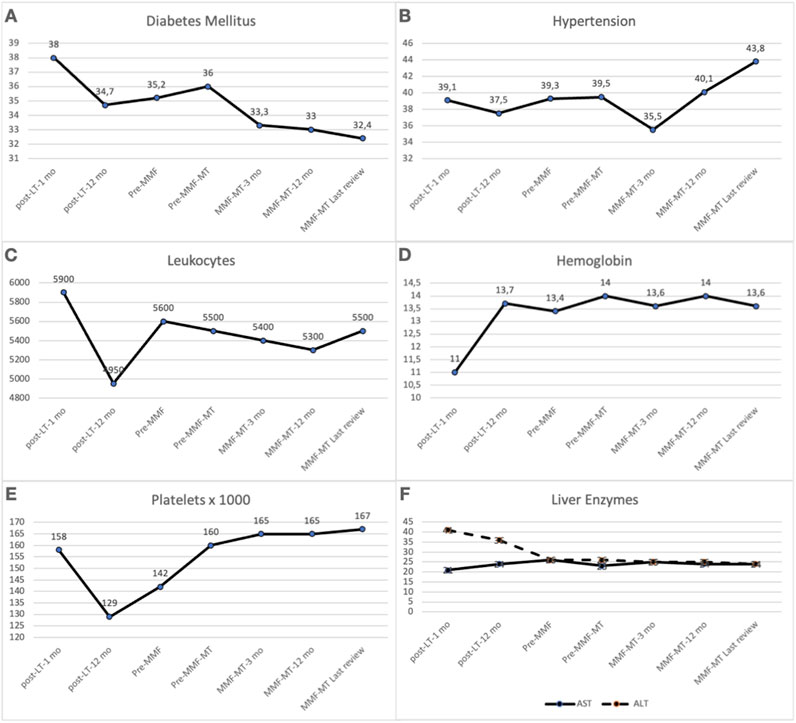
Figure 1. Comparison between the pre-MMF-MT period (combined MMF-CNI or CNI alone) and the final period of MMF-MT (last outpatient review) regarding the frequency of diabetes mellitus (A) (P = 0.603) and hypertension (B) (P = 0.141) and the median values of leukocytes (C) (P = 0.391), hemoglobin (D) (P = 0.115), platelets (E) (P = 0.210), AST (F) (P = 0.471) and ALT (F) (P = 0.106). *ALT, alanine amino transferase; AST, aspartate amino transferase; CNI, calcineurin inhibitor; GFR, glomerular filtration rate; MMF-MT, mycophenolate mofetil monotherapy.
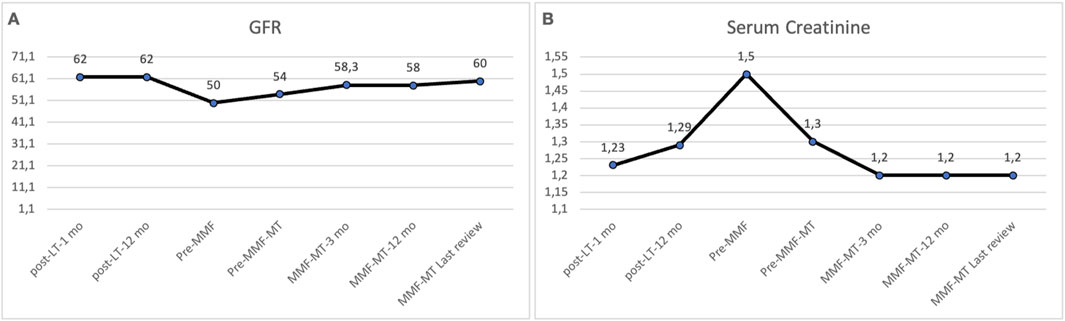
Figure 2. Comparison of renal function between the pre-MMF-MT period (combined MMF-CNI or CNI alone) and the final period of MMF-MT (last outpatient review). The median values of the GFR (A) increased significantly at the end of the study (56.5 mL/min/1.73 m2 vs. 61 mL/min/1.73 m2; p = 0.001). The median serum creatinine (B) value decreased at the end of the study, but the difference was not statistically significant (p = 0.112). *CNI, calcineurin inhibitor; GFR, glomerular filtration rate; MMF-MT, mycophenolate mofetil monotherapy.
Concerning comparison between both eras, we observed a significantly higher incidence of hypertension (p = 0.019) and diabetes mellitus (p = 0.023) before LT in the first era, and a significantly higher incidence of HCC (p < 0.001) in the second era, showing significant differences (p < 0.001) between the eras regarding indications of conversion to MMF-MT (Table 5).
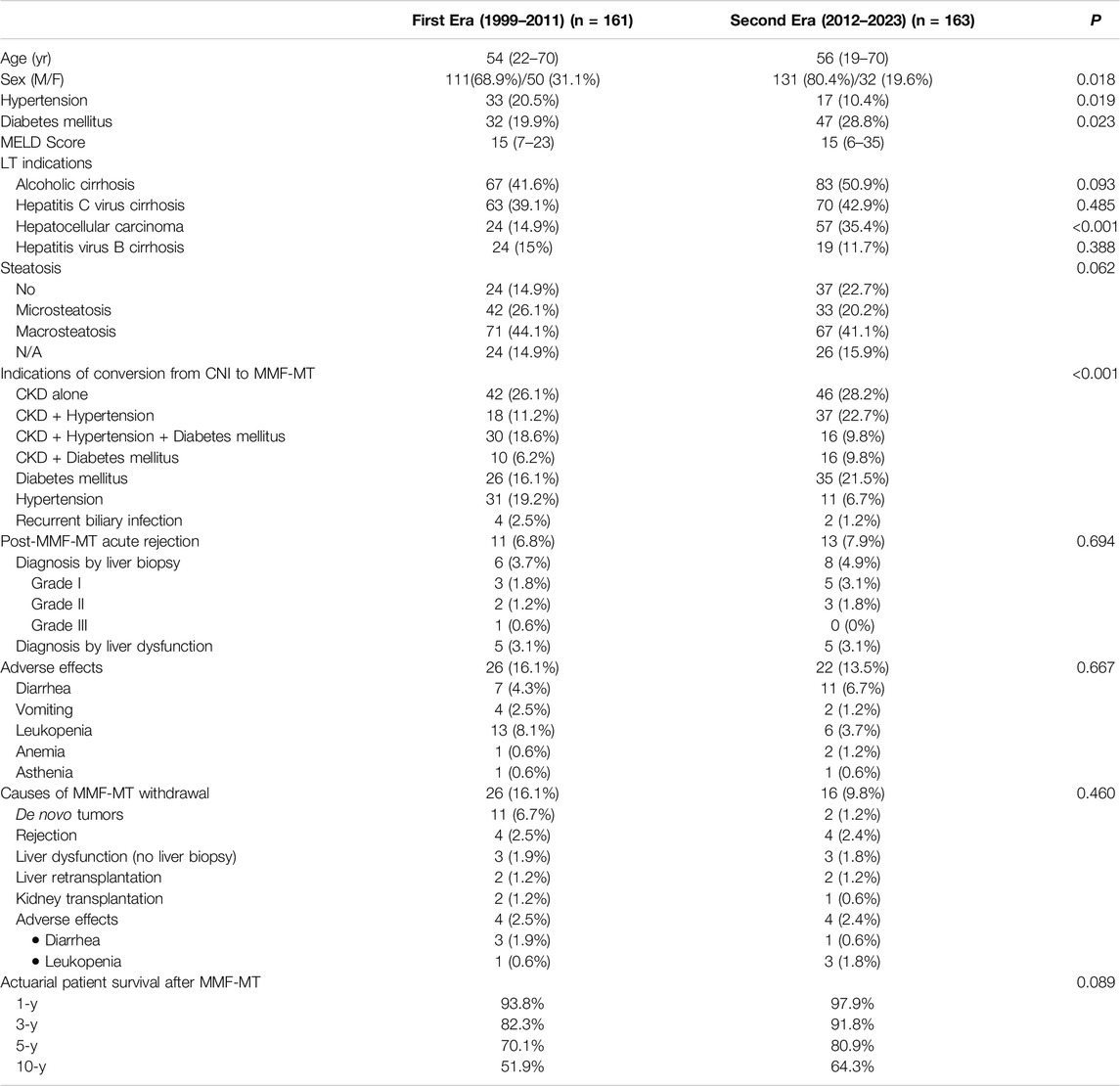
Table 5. Results according to eras of LT recipients converted from CNI to MMF-MT.
The overall actuarial patient survival rates at 1, 3, 5, and 10 years after the onset of MMF-MT were 95.7%, 86.5%, 75.3%, and 54.6%, respectively (Figure 3). The actuarial patient survival rate at 1, 3, 5, and 10 years after the onset of MMF-MT were 93.8%, 82.3%, 70.1%, and 51.9%, respectively, in era 1, whereas in the second era patient survival rate was 97.9%, 91.8%, 80.9%, and 64.3%, respectively. (p = 0.089) (Table 5).
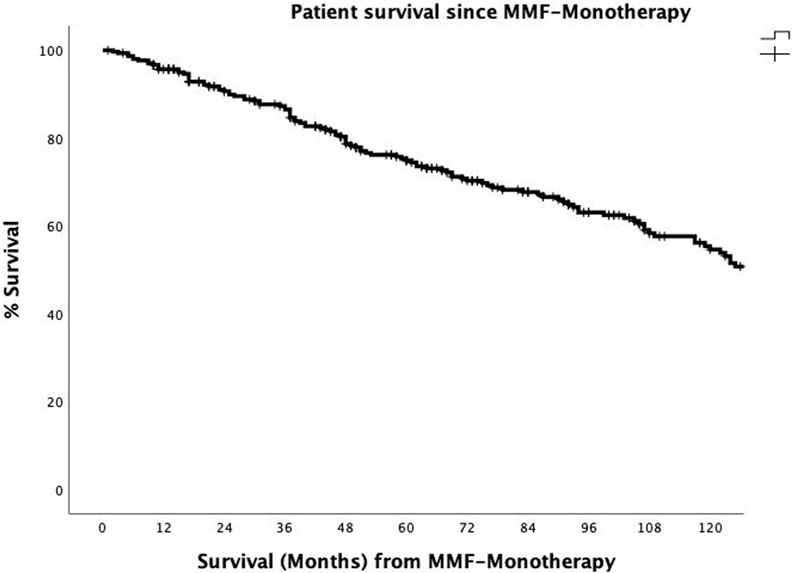
Figure 3. The actuarial patient survival rates after conversion from CNI immunosuppression to MMF-MT (mycophenolate mofetil monotherapy) at 1, 3, 5, and 10 years were 95.7%, 86.5, 75.3%, and 54.6%.
Discussion
The use of CNIs within the first 12 months after LT is a risk factor for renal failure [31], with a cumulative incidence of advanced CKD (GFR ≤29 mL/min) of 8% at 1 year and 18.1% at 5 years [32]. Renal function should improve more notably when the CNI is completely withdrawn than when it is partially withdrawn [33–35]. The substitution of CNI drugs for MMF-MT has been indicated mainly to halt or improve CKD and other CNI-induced adverse effects [16, 18, 19, 21–23, 33–35]. Other less frequent indications for shifting to MMF-MT were neurological or cardiovascular complications, risk of tumor recurrence [19], and metabolic disorders [18]. The most frequent indications for LT in our series were alcoholic cirrhosis, HCV, hepatitis B virus (HBV) and HCC, and tacrolimus was the most commonly used immunosuppressor, with an overall rate of acute rejection of 34.6% after LT. As in other reported studies [2–7], the main reasons for conversion from CNIs to MMF-MT in our study were the presence of CKD on its own or in association with diabetes or arterial hypertension and other adverse effects related to the use of CNIs, such as the presence of isolated diabetes, hypertension, or recurrent biliary infection.
Some researchers are reluctant to switch CNIs for MMF-MT in patients with previous history of graft rejection using CNIs [34], but the usual practice of other researchers is to switch CNI for MMF-MT in patients in the absence of acute rejection for 6–15 months before conversion [16, 17, 19, 36], the presence of stable liver function [16, 17, 21], and the absence of anemia, leukopenia and thrombocytopenia [36].
According to several studies, the time elapsed from LT to the onset of MMF-MT was between 27–81 months [16, 17, 19, 21, 22, 37–39], whereas in our experience, it corresponded to a median period of 72 months. The period of conversion from MMF-CNI to CNI withdrawal and the initiation of MMF-MT has been reported to last from 2 weeks to 9 months [16–19, 21, 25, 37, 40]; to 19 months in our experience. However, following our long-term experience, our period from the introduction of MMF to complete CNI withdrawal has been reduced to 1–2 months, with routine follow-up at 15, 30, and 90 days to detect occasional acute rejection or adverse effects.
The mean follow-up period of several studies of patients on MMF-MT is between 12 and 48 months [16–19, 21, 22, 38, 39], whereas our median follow-up time for patients on MMF-MT has reached 78 months.
Conversion from CNIs to MMF-MT is usually performed with an initial dose of 500 mg/12 h, reaching a dose of 1 g/12 h for 2–4 weeks simultaneously with a gradual reduction in CNI, usually by 25% at a time, until complete withdrawal [16, 17, 23, 25, 35]. Several authors have advised on maintaining MPA plasma levels between 1 and 3.5 ng/mL [41] or between 2 and 4 ng/mL, adjusting the MMF dosage according to the degree of renal dysfunction and monitoring of MPA plasma levels [21, 35, 39, 42, 43] because impaired renal function is correlated with a decrease in the clearance of MPA metabolites, which consequently increases the plasma concentration of MPA metabolites and augments immunosuppression [44]. Although MMF-MT may be a risk factor for liver rejection [45], we agree with other experiences that monitoring MPA levels can improve the management of immunosuppression [46] and may even limit the risk of rejection or drug toxicity [19, 23, 38, 45]. Thus, with MPA level monitoring, we adjusted the MMF doses between 500 and 2,000 mg/d to obtain median MPA levels between 2.5 and 3.3 ng/mL, maintaining 135 (38.6%) patients without rejection on a dose ≤1,000 mg/d of MMF at the last outpatient review. The monitoring of MPA levels allows the minimization of immunosuppression and prevents MMF-related adverse effects. However, AUC is considered the goal standard for measuring MPA levels [47], although in our experience it has been very impractical owing to the time and number of determinations it requires, especially among our high volume of patients, many of whom do not live in our city. Therefore, due to its simplicity and the need for only one determination per visit, it was decided in our center to use MPA levels.
Due to the mentioned risk of acute rejection, it is advisable to not attempt MMF-MT in poor MMF absorbers, which have been defined as patients with MPA levels <0.5 ng/mL after daily intake of ≥1,000 mg/d MMF or MPA levels <1 ng/mL after daily intake of 1,500 mg/d [48].
Substitution of CNIs by MMF-MMF has been associated with a rate of acute rejection ranging from 4% to 21.4% [16–19, 21, 22, 25, 37, 38, 48, 49]. Our rate of acute rejection was 7.4%, and as other researchers [23] have reported, diagnosis was performed either by liver biopsy or empirically by alteration of liver function. All our patients with acute rejection responded successfully with steroids and/or reintroduction of CNI or mTORi monotherapy, and no patients developed chronic rejection. However, late acute liver rejection can occur, and close follow-up during the first year after MMF-MT is advised, as has been previously reported [33].
The development of adverse effects is frequently related to MPA plasma levels higher than 4 ng/mL [41]. There is great variability in MMF-MT-induced side effects, ranging from an incidence between 4.3% and 57% [16, 17, 19, 21, 25, 37], although they are usually controlled by a reduction in the MMF dose [16, 18, 21, 35, 43], with the need for MMF-MT withdrawal in only 2%–11.8% of patients who show gastrointestinal symptoms, pancytopenia or pruritus [17, 19, 22, 25, 39]. In addition, gastrointestinal adverse effects can be improved by switching from MMF to enteric-coated mycophenolate sodium [50, 51]. In our study, 48 (14.8%) patients developed MMF-MT-induced adverse effects, but conversion to CNI was only performed in 8 (2.5%) patients due to failure to control severe diarrhea with enteric-coated mycophenolate sodium or leukopenia. The remaining adverse effects of patients improved when the dose of MMF decreased without the need to return to CNIs. Other reasons for MMT-MT withdrawal in our experience were the presence of de novo tumors (13 patients), biopsy-proven rejection or liver dysfunction (14 patients), liver retransplantation (4 patients) and kidney transplantation (3 patients).
Serum creatinine levels improved significantly in between 78.6% and 89% of the patients who were converted from CNIs to MMF-MT [16, 21, 25]. Similarly, replacement of CNIs with MMF-MT significantly increased the mean value of the GFR in patients with CKD [18, 19, 21, 22]. In our study, the comparison between the median values of the GFR in the pre-MMF-MT (CNI therapy) period and the last outpatient control, with a median value of 78 months between the two periods, revealed a significantly greater value of the GFR in the last control (56.5 vs. 61 mL/min/1.73 m2). The median serum creatinine value also improved at the last outpatient visit, but the difference was not statistically significant. However, when a repeated measures model was used taking each patient as its own comparator a significant increase of GFR and a significant decrease of serum creatinine and ALT values were demonstrated not showing significant differences regarding the rates of diabetes, hypertension, and values of hematological variables and AST.
In addition, the rates of diabetes mellitus and hypertension and the median values of hematological parameters (hemoglobin, leukocytes and platelets), serum glucose and liver transaminases did not significantly differ between the two periods. Notably, the 6 patients who were converted to MMF-MT due to recurrent cholangitis did not experience any more infection episodes after conversion. Five-year patient survival after conversion from CNI to MMF-MT was reported to be between 70% and 90% in 3 studies [19, 23, 35], and our 5-year patient survival rate was 75.3%. In the comparison of the results after conversion to MMF-MT in both eras we did not find significant differences regarding to the rates of acute rejection, adverse effects and causes of MMF-MT withdrawal, finding a higher patient survival rate in the second era, although statistically unsignificant.
This study has several limitations, such as its retrospective nature, long duration, and single institution design; consequently, it is subject to bias. Future multicenter prospective randomized studies with large samples are necessary to confirm our results.
In conclusion, MMF-MT can be safely used in LT patients with CNI-related adverse effects, such as CKD, hypertension, diabetes and biliary infection. Monitoring of MPA levels allows the reduction of the MMF dose and its adverse effects. The acute rejection rate was low, with a good response to CNI reintroduction or mTORi therapy, and the GFR, creatinine and ALT transaminase improved significantly through long-term follow-up. Comparison of the results between 2 eras did not show significant differences. A good tolerance of MMF-MT and a low rate of MMF-MT withdrawal have been shown.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics Statement
This study was approved by the institutional review board (approval number 24/025) and was conducted in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written informed consent participate in this study was not required due to the retrospective nature of the study.
Author Contributions
Study conceptualization and design (CJ-R, IJ, AMQ, and AMM). Acquisition of data (all authors). Data analysis (CJ-R, IJ, AMQ, OC, CL, FC, and CM-A). Data interpretation (CJ-R, IJ, AMQ, AMM, AG-S, JC, CL, CM-A, and AN). Writing of the original draft (CJ-R, IJ, and AMQ). Reviewing and editing (all authors). Supervision (CJ-R, IJ, and AMQ). All authors approved the submitted version.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank all the people involved in the abdominal organ transplantation program, specially to Inma Vidal and Esther Clemente.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontierspartnerships.org/articles/10.3389/ti.2025.13790/full#supplementary-material
Abbreviations
ALT, alanine amino transferase; AST, aspartate amino transferase; BMI, body mass index; CKD, chronic kidney disease; CNI, calcineurin inhibitor; DBD, donation after brain death; GFR, glomerular filtration rate; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; LT, liver transplantation; MELD, model for end-stage liver disease; MMF, mycophenolate mofetil; MT, monotherapy; MPA, mycophenolic acid.
References
1. Charlton, M, Levitsky, J, Aqel, B, O´Grady, J, Hemibach, J, Rinella, M, et al. International Liver Transplantation Society Consensus Statement on Immunosuppression in Liver Transplant Recipients. Transplantation (2018) 102:727–43. doi:10.1097/TP.0000000000002147
2. Klupp, J, Pfitzmann, R, Langrehr, JM, and Neuhauss, P. Indications of Mycophenolate Mofetil in Liver Transplantation. Transplantation (2005) 80:S142–6. doi:10.1097/01.tp.0000187133.53916.8f
3. Morard, I, Mentha, G, Spahr, L, Majno, P, Hadengue, A, Huber, O, et al. Long-Term Renal Function After Liver Transplantation Is Related to Calcineurin Inhibitors Blood Levels. Clin Transpl (2006) 20:96–101. doi:10.1111/j.1399-0012.2005.00447.x
4. Ojo, AO. Renal Disease in Recipients of Nonrenal Solid Organ Transplantation. Semin Nephrol (2007) 27:498–507. doi:10.1016/j.semnephrol.2007.03.010
5. Kuo, HT, Sampaio, MS, Ye, X, Reddy, P, Martin, P, and Bunnapradist, S. Risk Factors for New-Onset Diabetes Mellitus in Adult Liver Transplant Recipients, an Analysis of the Organ Procurement and Transplant Network/United Network for Organ Sharing Database. Transplantation (2010) 89:1134–40. doi:10.1097/TP.0b013e3181d2fec1
6. Rodríguez-Perálvarez, M, Germani, G, Darius, T, Lerut, J, Tsochatzis, E, and Burroughs, AK. Tacrolimus Through Levels, Rejection and Renal Impairment in Liver Transplantation. A Systematic Review and Meta-Analysis. Am J Transpl (2012) 12:2797–814. doi:10.1111/j.1600-6143.2012.04140.x
7. Carenco, C, Assenat, E, Faure, S, Duny, Y, Danan, G, Bismuth, M, et al. Tacrolimus and the Risk of Solid Cancers After Liver Transplant: A Dose Effect Relationship. Am J Transpl (2015) 15:678–86. doi:10.1111/ajt.13018
8. Karie-Guigues, S, Janus, N, Saliba, F, Dumortier, J, Duvaux, C, Calmus, Y, et al. Long-Term Renal Function in Liver Transplantation Recipients and Impact of Immunosuppressive Regimens [Calcineurin Inhibitors Alone or in Combination With Mycophenolate Mofetil]:The TRY Study. Liver Transpl (2009) 15:1083–91. doi:10.1002/lt.21803
9. Hao, JC, Wang, WT, Yan, LN, Li, B, Wen, TF, Jang, JY, et al. Effect of Low-Dose Tacrolimus With Mycophenolate Mofetil on Renal Function Following Liver Transplantation. World J Gastroenterol (2014) 20:11356–62. doi:10.3748/wjg.v20.i32.11356
10. Duvoux, C, and Pageaux, GP. Immunosuppression in Liver Transplant Recipients With Renal Impairment. J Hepatol (2011) 54:1041–54. doi:10.1016/j.jhep.2010.12.001
11. Jimenez-Romero, C, Manrique, A, Marqués, E, Calvo, J, García-Sesma, A, Cambra, F, et al. Switching to Sirolimus Monotherapy for De Novo Tumors After Liver Transplantation. A Preliminary Experience. Hepatogastroenterology (2011) 58:115–21.
12. Alegre, C, Jiménez, C, Manrique, A, Abradelo, M, Calvo, J, Loinaz, C, et al. Everolimus Monotherapy or Combined Therapy in Liver Transplantation: Indications and Results. Transpl Proc (2013) 45:1971–4. doi:10.1016/j.transproceed.2013.01.075
13. Saliba, F, Duvoux, C, Guhengein, J, Kamar, N, Dharancy, S, Salamé, E, et al. Efficacy and Safety of Everolimus and Mycophenolic Acid With Early Tacrolimus Withdrawal After Liver Transplantation: A Multicenter Randomized Trial. Am J Transpl (2017) 17:1843–53. doi:10.1111/ajt.14212
14. Orlando, G. Finding the Right Time for Weaning off Immunosuppression in Solid Organ Transplant Recipients. Exp Rev Clin Immunol (2010) 6:879–92. doi:10.1586/eci.10.71
15. Londoño, MC, Rimola, A, O´Grady, J, and Sanchez-Fueyo, A. Immunosuppression Minimization vs Complete Drug Withdrawal in Liver Transplantation. J Hepatol (2013) 59:872–9. doi:10.1016/j.jhep.2013.04.003
16. Moreno, JM, Cuervas-Mons, V, Rubio, E, Gómez, A, López-Monclus, J, Sánchez-Turrión, V, et al. Mycophenolate Mofetil Can Be Used as Monotherapy Late After Liver Transplantation. Am J Transpl (2004) 4:1650–5. doi:10.1111/j.1600-6143.2004.00556.x
17. Manrique, A, Jiménez, C, Ortega, P, Abradelo, M, Gimeno, A, Calvo, J, et al. Mycophenolate Mofetil Monotherapy in Patients Who Underwent Liver Transplantation for Hepatitis C Cirrhosis. Transpl Proc (2008) 40:2962–4. doi:10.1016/j.transproceed.2008.09.040
18. Dharancy, S, Iannelli, A, Hulin, A, Declerck, N, Schneck, AS, Mathurin, P, et al. Mycophenolate Mofetil Monotherapy for Severe Side Effects of Calcineurin Inhibitors Following Liver Transplantation. Am J Transpl (2009) 9:610–3. doi:10.1111/j.1600-6143.2008.02529.x
19. Lassailly, G, Dumortier, J, Saint-Marcoux, F, El Amrani, M, Boulanger, J, Boleslawski, E, et al. Real Life Experience of Mycophenolate Mofetil Monotherapy in Liver Transplant Patients. Clin Res Hepatol Gastroenterol (2021) 45:101451. doi:10.1016/j.clinre.2020.04.017
20. McKay, DB, and Josephson, MA. Pregnancy in Recipients of Solid Organs-Effects on Mother and Child. N Engl J Med (2006) 354:1281–93. doi:10.1056/NEJMra050431
21. Orlando, G, Baiocchi, L, Cardillo, A, Iaria, G, De Liguori Carino, N, De Luca, L, et al. Switch to 1.5 Grams MMF Monotherapy for CNI-Related Toxicity in Liver Transplantation Is Safe and Improves Renal Function, Dyslipidemia, and Hypertension. Liver Transpl (2007) 13(1):46–54. doi:10.1002/lt.20926
22. Kriss, M, Sotil, EU, Abecassis, M, Welti, M, and Levitsky, J. Mycophenolate Mofetil Monotherapy in Liver Transplant Recipients. Clin Transpl (2011) 25:E639–46. doi:10.1111/j.1399-0012.2011.01512.x
23. Schmeding, M, Kiessling, A, Neuhaus, R, Heidenhain, C, Bahra, M, Neuhaus, P, et al. Mycophenolate Mofetil Monotherapy in Liver Transplantation: 5-Year Follow-Up of a Prospective Randomized Trial. Transplantation (2011) 92:923–9. doi:10.1097/TP.0b013e31822d880d
24. Cruz, CM, Pereira, S, Gandara, J, Ferreira, S, Lopes, V, Daniel, J, et al. Efficacy and Safety of Monotherapy With Mycophenolate Mofetil in Liver Transplantation Patients With Nephrotoxicity. Transpl Proc (2016) 48:2341–3. doi:10.1016/j.transproceed.2016.06.033
25. Schlitt, HJ, Barkmann, A, Boker, KHW, Schmidt, HHJ, Emmanouilidis, N, Rosenau, J, et al. Replacement of Calcineurin Inhibitors With Mycophenolate Mofetil in Liver-Transplant Patients with Renal Dysfunction: A Randomized Controlled Study. Lancet (2001) 357:587–91. doi:10.1016/s0140-6736(00)04055-1
26. Watt, KD, and Charlton, MR. Metabolic Syndrome and Liver Transplantation: A Review and Guide to Management. J Hepatol (2010) 53:199–206. doi:10.1016/j.jhep.2010.01.040
27. Levey, AS, Stevens, LA, Schmid, CH, Zhang, YL, Castro, 3rd AF, Feldman, HI, et al. A New Equation to Estimate Glomerular Filtration Rate. Ann Int Med (2009) 150:604–12. doi:10.7326/0003-4819-150-9-200905050-00006
28. Bakris, G, Ali, W, and Parati, G. ACC/AHA versus ESC/ESH on Hypertension Guidelines. JACC Guidelines Comparison. J Am Coll Cardiol (2019) 73:3018–26. doi:10.1016/j.jacc.2019.03.507
29. American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care (2020) 43(Suppl. 1):S14–S31. doi:10.2337/dc20-S002
30. Demetris, AJ, Batts, KP, Dhillon, AP, Ferrell, L, Fung, J, Geller, SA, et al. Banff Schema for Grading Liver Allograft Rejection: An International Consensus Document. Hepatology (1997) 25:658–63. doi:10.1002/hep.510250328
31. Wilkinson, A, and Pham, PT. Kidney Dysfunction in the Recipients of Liver Transplants. Liver Transpl (2005) 11:S47–S51. doi:10.1002/lt.20618
32. Ojo, AO, Held, PJ, Port, FK, Wolfe, RA, Leichtman, AB, Young, EW, et al. Chronic Renal Failure After Transplantation of a Nonrenal Organ. N Engl J Med (2003) 349:931–40. doi:10.1056/NEJMoa021744
33. Reich, DJ, Clavien, PA, and Hodge, EE, MMF Renal Dysfunction After Liver Transplantation Working Group. Mycophenolate Mofetil for Renal Dysfunction in Liver Transplant Recipients on Cyclosporine or Tacrolimus: Randomized, Prospective, Multicenter Pilot Study Results. Transplantation (2005) 80:18–25. doi:10.1097/01.tp.0000165118.00988.d7
34. Creput, C, Blandin, F, Deroure, B, Roche, B, Saliba, F, Charpentier, B, et al. Long-Term Effects of Calcineurin Inhibitor Conversion to Mycophenolate Mofetil on Renal Function After Liver Transplantation. Liver Transpl (2007) 13:1004–10. doi:10.1002/lt.21170
35. Bilbao, I, Castells, L, Rojas, L, Cancino, J, Dopazo, C, Castro, E, et al. Immunosuppression Based on Mycophenolate Mofetil in Stable Liver Transplanted Patients. Int Immunopharmacol (2006) 6:1977–83. doi:10.1016/j.intimp.2006.09.022
36. Herrero, JI, Quiroga, J, Sangro, B, Pardo, F, Rotellar, F, Cienfuegos, JA, et al. Conversion From Calcineurin Inhibitors to Mycophenolate Mofetil in Liver Transplant Recipients With Diabetes Mellitus. Transpl Proc (2003) 35:1877–9. doi:10.1016/s0041-1345(03)00644-4
37. Raimondo, ML, Dagher, L, Papatheodoridis, GV, Rolando, N, Patch, DW, Davidson, BR, et al. Long-Term Mycophenolate Mofetil Monotherapy in Combination With Calcineurin Inhibitors for Chronic Renal Dysfunction After Liver Transplantation. Transplantation (2003) 75:186–90. doi:10.1097/01.TP.0000041702.31262.CD
38. Fairbanks, D, and Thuluvath, PJ. Mycophenolate Mofetil Monotherapy in Liver Transplant Recipients: A Single Center Experience. Liver Transpl (2004) 10:1189–94. doi:10.1002/lt.20210
39. Jiménez-Pérez, M, Lozano Rey, JM, Marín García, D, Olmedo Martín, R, de la Cruz Lombardo, J, and Rodrigo López, JM. Efficacy and Safety of Monotherapy With Mycophenolate Mofetil in Liver Transplantation. Transpl Proc (2006) 38:2480–1. doi:10.1016/j.transproceed.2006.08.039
40. Pierini, A, Mirabella, S, Brunati, A, Ricchiuti, A, Franchello, A, and Salizzoni, M. Mycophenolate Mofetil Monotherapy in Liver Transplantation. Transpl Proc (2005) 37:2614–5. doi:10.1016/j.transproceed.2005.06.005
41. Tredger, JM, Brown, NW, Adams, J, Gonde, CE, Dhawan, A, Rela, M, et al. Monitoring Mycophenolate in Liver Transplant Recipients: Toward a Therapeutic Range. Liver Transpl (2004) 10:492–502. doi:10.1002/lt.20124
42. Park, YH, Hwang, S, Song, GW, Jung, DH, Ahn, CS, Kim, KH, et al. Correlation Between Mycophenolic Acid Blood Level and Renal Dysfunction in Stable Liver Transplant Recipients Receiving Mycophenolate Monotherapy. Transpl Proc (2014) 46:811–5. doi:10.1016/j.transproceed.2013.12.042
43. Hwang, S, Ahn, CS, Kim, KH, Moon, DB, Ha, TY, Son, GW, et al. A Cross-Sectional Analysis of Long-Term Immunosuppressive Regimens After Liver Transplantation at Asan Medical Center: Increased Preference for Mycophenolate Mofetil. Ann Hepatobiliary Pancreat Surg (2018) 22:19–26. doi:10.14701/ahbps.2018.22.1.19
44. Jain, A, Venkataramanan, R, Hamad, IS, Zuckerman, S, Zhang, S, Lever, J, et al. Pharmacokinetics of Mycophenolic Acid After Mycophenolate Mofetil Administration in Liver Transplant Patients Treated With Tacrolimus. J Clin Pharmacol (2001) 41:268–76. doi:10.1177/00912700122010087
45. Brunet, M, Cirera, I, Martorell, J, Vidal, E, Millán, O, Jiménez, O, et al. Sequential Determination of Pharmacokinetics and Pharmacodynamics of Mycophenolic Acid in Liver Transplant Patients Treated With Mycophenolate Mofetil. Transplantation (2006) 81:541–6. doi:10.1097/01.tp.0000200307.79962.48
46. Tredger, JM, and Brown, NW. Mycophenolate: Better Value Through Monitoring? Transplantation (2006) 81:507–8. doi:10.1097/01.tp.0000200308.21816.53
47. Bergan, S, Brunet, M, Hesselink, DA, Johnson-Davis, KL, Kunicki, PK, Lemaitre, F, et al. Personalized Therapy for Mycophenolate: Consensus Report by the International Association of Therapeutic Drug Monitoring and Clinical Toxicology. The Drug Monit (2021) 43:150–200. doi:10.1097/FTD.0000000000000871
48. Hwang, S, Lee, SG, Ahn, CS, Kim, KH, Moon, DB, Ha, TY, et al. A Clinical Assessment of Mycophenolate Drug Monitoring After Liver Transplantation. Clin Transpl (2010) 24:E35–E42. doi:10.1111/j.1399-0012.2009.01166.x
49. Goralczyk, A, Bari, N, Abu-Ajaj, W, Lorf, T, Ramadori, G, Friede, T, et al. Calcineurin Inhibitor Sparing With Mycophenolate Mofetil in Liver Transplantation: A Systematic Review of Randomized Controlled Trials. Am J Transpl (2012) 12:2601–7. doi:10.1111/j.1600-6143.2012.04157.x
50. Dumortier, J, Gagnieu, MC, Salandre, J, Guillaud, O, Guillem, P, Adham, M, et al. Conversion From Mycophenolate Mofetil to Enteric-Coated Mycophenolate Sodium in Liver Transplant Patients Presenting Gastrointestinal Disorders: A Pilot Study. Liver Transpl (2006) 12:1342–6. doi:10.1002/lt.20792
51. Toledo, AH, Hendrix, L, Buchholz, V, Fisher, E, Newton, K, Smith, C, et al. Improvement of Gastrointestinal Symptoms After Conversion From Mycophenolate Mofetil to Enteric-Coated Mycophenolate Sodium in Liver Transplant Patients. Clin Transpl (2012) 26:156–63. doi:10.1111/j.1399-0012.2011.01444.x
Keywords: mycophenolate mofetil, tacrolimus, cyclosporine, immunosuppression minimization, liver transplantation, chronic kidney dysfunction
Citation: Jiménez-Romero C, Justo Alonso I, Caso Maestro O, Manrique Municio A, García-Sesma Á, Calvo Pulido J, Cambra Molero F, Loinaz Segurola C, Martín-Arriscado C, Nutu A and Marcacuzco Quinto A (2025) Indications and Long-Term Outcomes of Using Mycophenolate Mofetil Monotherapy in Substitution for Calcineurin Inhibitors in Liver Transplantation. Transpl Int 38:13790. doi: 10.3389/ti.2025.13790
Received: 12 September 2024; Accepted: 27 January 2025;
Published: 21 February 2025.
Copyright © 2025 Jiménez-Romero, Justo Alonso, Caso Maestro, Manrique Municio, García-Sesma, Calvo Pulido, Cambra Molero, Loinaz Segurola, Martín-Arriscado, Nutu and Marcacuzco Quinto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Iago Justo Alonso, aWp1c3RvQHVjbS5lcw==
†These authors have contributed equally to this work