 Sofia El Hajji1,2*
Sofia El Hajji1,2* Stéphanie Lacotte1,2
Stéphanie Lacotte1,2 Beat Moeckli1,2†François Cauchy1
Beat Moeckli1,2†François Cauchy1 Philippe Compagnon1,3
Philippe Compagnon1,3 Christian Toso1,2,3*
Christian Toso1,2,3*- 1Division of Abdominal Surgery, Department of Surgery, Geneva University Hospitals, Geneva, Switzerland
- 2Laboratory of Transplantation and Hepatology, University of Geneva, Geneva, Switzerland
- 3Division of Transplantation, Department of Surgery, Geneva University Hospitals, Geneva, Switzerland
Transjugular intrahepatic portosystemic shunt (TIPS) reduces portal hypertension complications. Its impact on hepatocellular carcinoma (HCC) remains unclear. We evaluated 42,843 liver transplant candidates with HCC from the Scientific Registry of Transplant Recipients (2002–2022). 4,484 patients with and without TIPS were propensity score-matched 1:3. Analysing wait-list changes in total tumor volume, HCC count, and alpha-fetoprotein levels, and assessing survival from listing and transplantation; TIPS correlated with a decreased nodule count (−0.24 vs. 0.04, p = 0.028) over a median wait period of 284 days (IQR 195–493) and better overall survival from listing (95.6% vs. 91.5% at 1 year, p < 0.0001). It was not associated with changes in tumor volume (0.28 vs. 0.11 cm³/month, p = 0.58) and AFP (14.37 vs. 20.67 ng/mL, p = 0.42). Post-transplant survival rates (91.8% vs. 91.7% at 1 year, p = 0.25) and HCC recurrence (5.1% vs. 5.9% at 5 years, p = 0.14) were similar, with a median follow-up of 4.98 years (IQR 2.5–8.08). While TIPS was associated with a reduced nodule count and improved waitlist survival, it did not significantly impact HCC growth or aggressiveness. These findings suggest potential benefits of TIPS in HCC management, but further studies need to confirm TIPS safety.
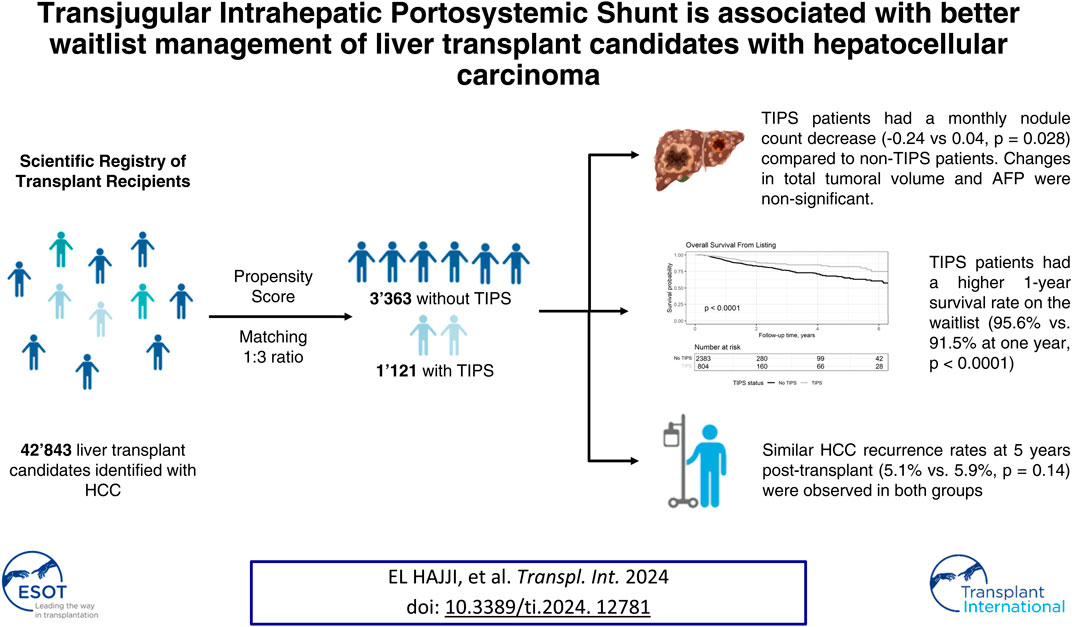
GRAPHICAL ABSTRACT | Created with Biorender.com.
Introduction
Transjugular intrahepatic portosystemic shunt (TIPS) is a valuable interventional strategy to alleviate portal hypertension complications. It effectively diverts blood flow from the portal vein to the hepatic veins, lowering portal pressure and its subsequent clinical manifestations including ascites and variceal bleeding [1, 2]. Despite its clinical advantages in portal hypertension, the role of TIPS in the management of patients remains unclear [3, 4]. Some authors have revealed no association between TIPS and de novo HCC nodules, while others caution against a potentially increased risk of HCC occurrence [5–8]. Concerns regarding the potential influence on tumor behavior persist, especially considering the limited sample sizes of many studies. Alterations in hepatic blood flow dynamics could theoretically promote tumor growth or metastasis through various mechanisms, including hypoxic liver injury, dissemination at insertion, or reduced response to locoregional treatment [9, 10].
We took advantage of a large prospective database from the Scientific Registry of Transplant Recipients (SRTR), which includes mandatory data from all liver transplant candidates in the United States. While on the list, HCC patients undergo periodic imaging and alpha-fetoprotein (AFP) assessments to benefit from exception Model for End-Stage Liver Disease (MELD) points. This dataset granted us access to data on HCC characteristics, such as size, number, and AFP, while patients were on the waitlist. Our study focused on comparing patients with and without TIPS at the time of listing to elucidate its impact on the progression of HCC.
Materials and Methods
Study Population
This study utilized data from the SRTR database, a prospective registry that contains information on all donors, wait-listed candidates, and transplant recipients in the United States. The SRTR registry, submitted by members of the Organ Procurement and Transplantation Network (OPTN), encompasses a comprehensive list of patients registered from February 01, 2002, which corresponds to MELD implementation in the United States, to June 2, 2022, date of data retrieving.
Our study selected patients diagnosed with HCC as their primary or secondary diagnosis and compared them with (1,132) versus without TIPS (21,393) at the time of listing. Patients with liver tumors other than HCC were also excluded from the study. The TIPS status was determined prior to listing using the “CAN_TIPSS” label. We aimed to investigate the variations in HCC characteristics among patients on the waiting list for transplantation.
Data Collection
Data management and analysis were conducted using the R studio software (version 2022.07.2 + 576) [11]. Patient characteristics included age, sex, body mass index (BMI), underlying liver disease diagnosis, date of listing, date of transplantation, date of death, and time of follow-up. We classified the underlying liver diseases as viral, non-alcoholic steatohepatitis (NASH), and alcoholic liver disease (OH). An “other” category encompassing less prevalent etiologies like metabolic disease, cholestatic disease, drug exposure, and autoimmune disorders, each constituting less than 5% of the studied population. MELD was calculated in accordance with the 2016 revision by the United Network for Organ Sharing using a custom R function that assigned a minimum value of 1 to any log-scaled values less than 1 to prevent negative scores. Sodium levels were capped between 125 and 137 mg/dL, whereas creatinine levels were capped at 4 mmol/L. The maximum attainable MELD score was 40.
We collected HCC characteristics at each MELD exception update from the “MPEXCEPT” list, allowing longitudinal monitoring of each patient. The characteristics included the HCC diameter, count, and AFP levels. For patients with multiple HCCs, the total tumor volume (TTV) was calculated by summing the volumes (calculated as the volume of a sphere V = 4/3πr³) of the individual HCCs. The tumor burden was also evaluated based on the number of tumors. We assessed changes in TTV and tumor count between the first (at listing) and last (or pre-transplant) assessments, measuring changes per patient in volume in cm³ per month and count in units per year. Changes in AFP levels were expressed in ng/mL per month. In terms of therapeutic interventions, HCC treatments were categorized as: “curative” when cryotherapy, thermoablation, chemical ablation, or surgery were used; “locoregional chemotherapy” when chemoembolization was used; “mixed” when both modalities were used; or “untreated” in the absence of HCC-directed treatment.
Propensity Score Matching
Propensity score matching (PSM) was performed using the “MatchIt” package to achieve covariate balance and mitigate selection bias between groups with and without TIPS [12]. Prior to performing the matching, we ensured that only patients with complete data for the matching criteria and their outcomes were evaluated. Matching utilized nearest-neighbor matching with a 3:1 pairing ratio to optimize the analysis. Patients were matched based on age, body mass index (BMI), underlying liver disease, initial calculated TTV, nodule count, AFP levels, waitlist HCC treatment category, and the calculated MELD score. The aim of this study was to minimize differences in liver function and initial HCC characteristics between the TIPS and non-TIPS groups to better capture the effect of TIPS on HCC, including TTV, nodule count, and AFP levels.
Statistical Analysis
Survival was first evaluated from listing by censoring transplanted patients in the matched cohort. Post-transplant survival was then studied in patients who eventually underwent transplantation from the matched cohort. We used the listing date, transplantation date, and death date to compute the survival curves. Post-transplant HCC recurrence was determined following a procedure previously used by our group and others in the same cohort [13, 14]. Notably, this procedure provides an accurate assessment of recurrence rate.
Statistical analyses were conducted using the R Studio software. The analytical results were visualized using the “gtsummary” package [15]. To compare sample distributions, we employed the Welch two-sample t-test, Wilcoxon test, and Pearson’s chi-squared test. For survival analysis, we utilized both the “survival” and “survminer” packages [16, 17]. The Kaplan-Meier method was used to assess overall survival (OS), and differences between groups were assessed using the log-rank test. The cumulative incidence risk of HCC was calculated using the “tidycmprsk” package, and the differences were compared using Gray’s test [18]. Statistical significance was set at a threshold of p < 0.05.
Results
Demographics
During the study period (data dating back from February 1, 2002, until June 2, 2022), a total of 42,843 patients diagnosed with HCC were placed on the waiting list. Patient characteristics are reported in Table 1, and the measured outcomes of HCC progression are shown in Table 2. Patients with TIPS were younger, had a higher BMI, and had a higher prevalence of alcohol-related liver disease. These patients also displayed more advanced liver disease, as indicated by higher Model for MELD scores, but less advanced HCC staging as shown by their TTV et number of tumors at listing.
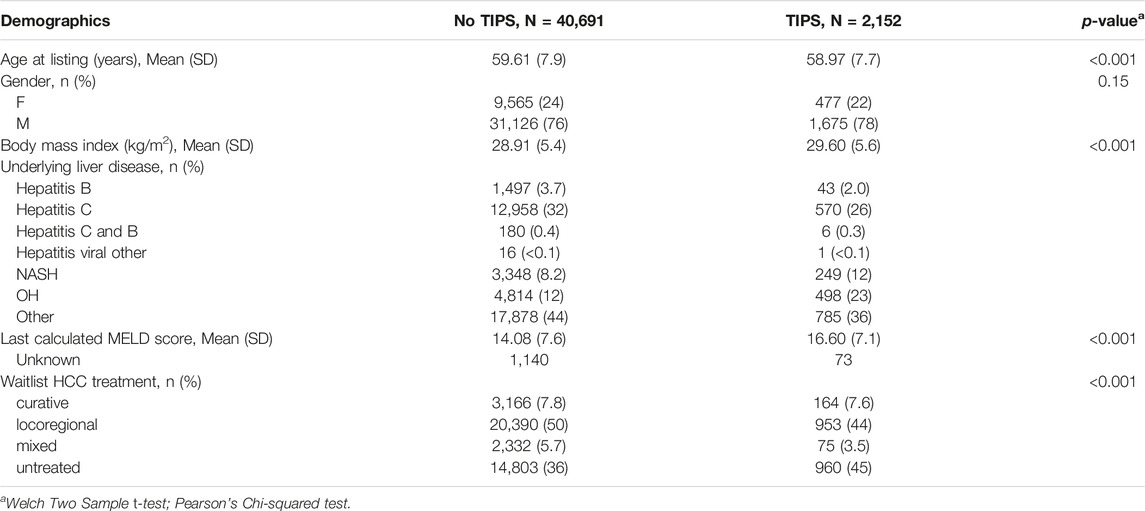
Table 1. Demographics of the selected HCC patients compared between patients with (TIPS) and without (No TIPS) a history of TIPS.
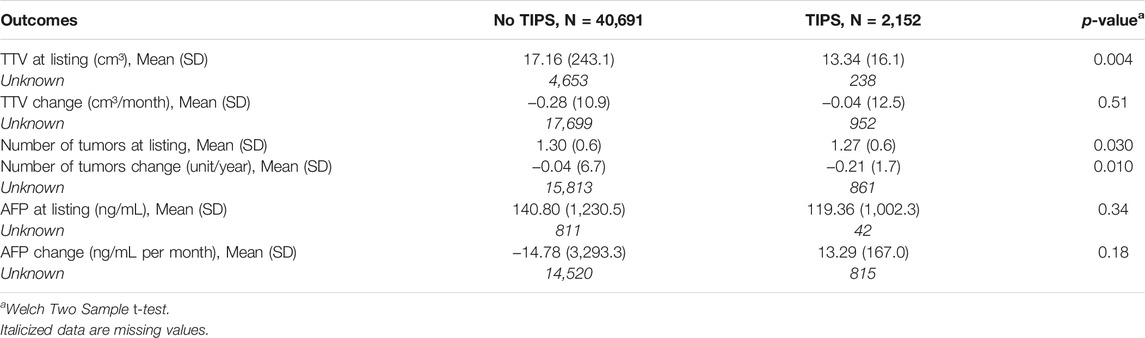
Table 2. Outcomes on HCC evolution measured on the whole cohort and compared between patients with and without TIPS.
Propensity Score Matching
Considering the disparities between the groups, we implemented propensity score matching to equilibrate the data. This approach allowed us to investigate the specific effects of TIPS on HCC volume, number, and AFP changes over a median waiting time 284 days (IQR 195–493). The matching process was performed on a 3:1 basis and accounted for the covariates described in the Methods section. The balanced data are presented in Table 3.
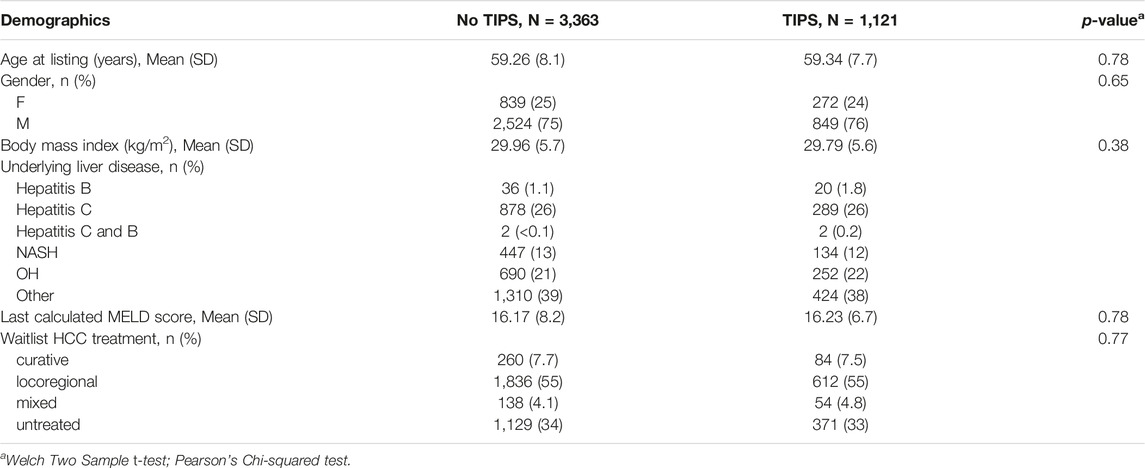
Table 3. Balanced table of the matched cohort.
HCC-Related Data
Following propensity matching, the HCC characteristics between patients with and without TIPS did not reach statistical significance anymore, as outlined in Table 4, this was done to match the patients on tumor biology as closely as possible. We then explored the waitlist changes to capture the effect of TIPS on HCC progression. A negative change in HCC volume or count indicates an effective tumor treatment or resection. Conversely, a positive monthly change was indicative of ineffective treatment (or absence of treatment) and/or more aggressive HCC.

Table 4. Outcomes on HCC evolution after matching.
TIPS was associated with a decrease in the number of HCC, potentially indicating more efficient treatment of these lesions. There were no significant changes in volume or AFP dynamics between the groups as presented in Table 4.
Of note, we also performed a sensitivity analysis, also including patients with missing data. Similar outcomes have been observed, with a decrease in the number of HCC, and no change in volume and AFP dynamics (data not shown).
Overall Survival From Listing
We compared overall survival (OS) from listing between patients with and without TIPS in the matched cohort. OS at 1, 5, and 10 years accounted for 95.6%, 82.1%, and 66%, respectively, in the TIPS and 91.5%, 65.1%, and 52%, respectively, in the no-TIPS group (log-rank test: p < 0.0001), as shown in Figure 1. Despite a longer waiting time to transplant for the TIPS group, which was 324 days (IQR 210; 607) compared to 272 days (IQR 191; 463) for the non-TIPS group (Wilcoxon test p < 0.001), survival rates were notably higher in the TIPS group.
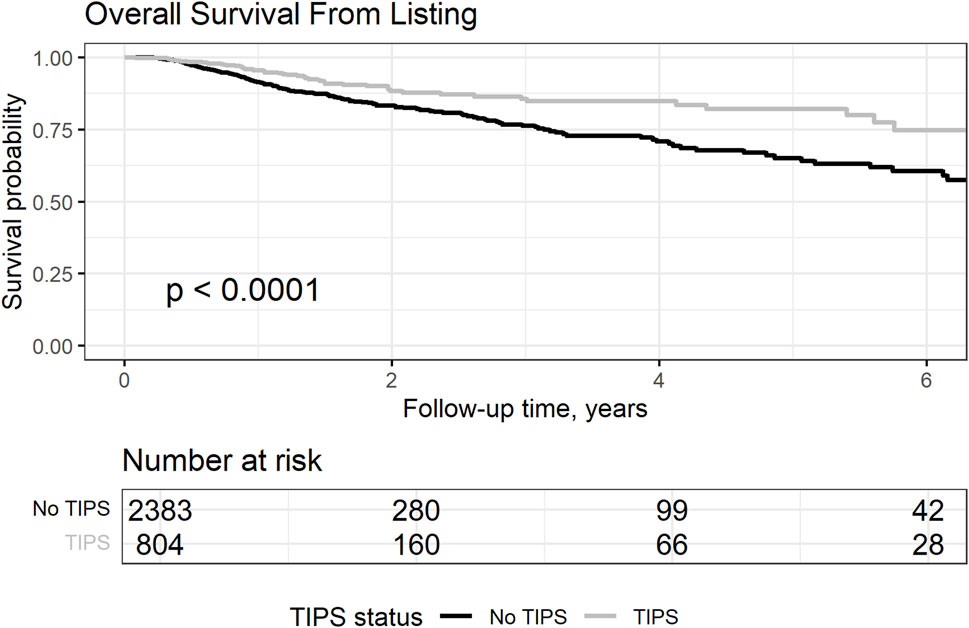
Figure 1. Overall survival from listing in the matched cohort, censoring transplanted patients and comparing patients with and without TIPS.
We further explored the causes of the observed differences in the survival rates. Removal from the waitlist concerned 26% (N = 268) of TIPS and 24% (N = 888) of non-TIPS patients. Among them, 50% (N = 135) of TIPS vs. 46% (N = 408) of non-TIPS patients were too ill to be transplanted, and 23% (N = 56) of TIPS vs. 29% (N = 224) of non-TIPS patients died. When exploring the causes of death, hemorrhage-related death was more frequent in the non-TIPS group (1.8%, N = 1 in TIPS and 7.6%, N = 17 in non-TIPS patients).
Post-Transplantation Outcomes
Analysis of post-transplant overall survival rates revealed no statistically significant difference between patients with and without TIPS (Figure 2). At 1, 5, and 10 years post-transplant, survival rates were comparable between the TIPS (92.6%, 79.6%, and 68.8%, respectively) and no-TIPS group (93.4%, 78.3%, and 67.1%, respectively, p = 0.39). The time of follow-up from listing was also similar (5.14 versus 4.88 years, p = 0.14). These results suggest that TIPS does not affect post-transplantation survival in patients with HCC, which aligns with previous data [19, 20].
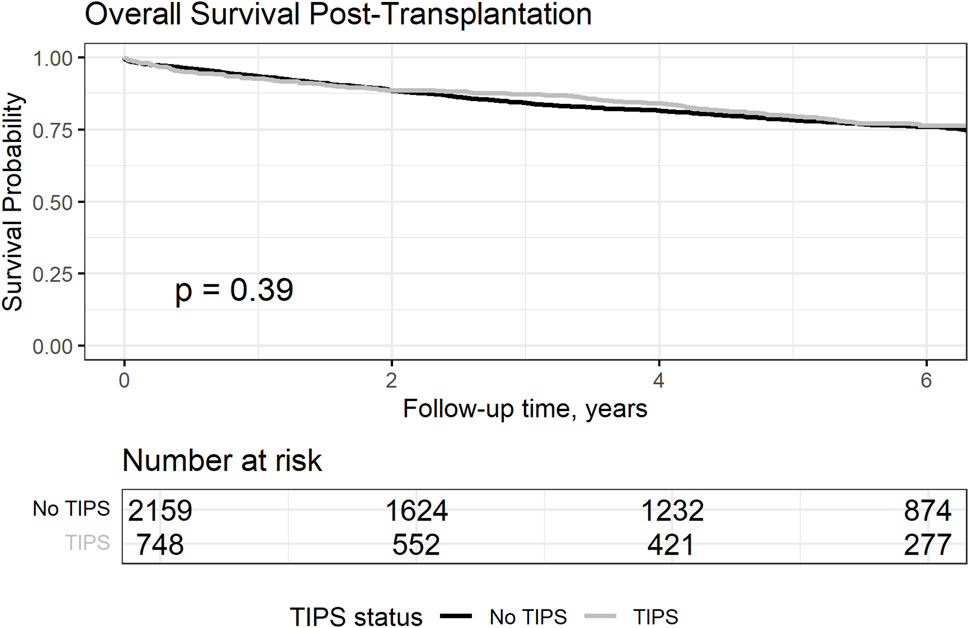
Figure 2. Overall survival from transplantation in the matched cohort comparing patient with and without TIPS.
Considering the observed HCC dynamics while on the waitlist, we further explored whether this could have an impact on the risk of posttransplant HCC recurrence (Figure 3). The cumulative risk incidence of post-transplant HCC recurrence at 5 years was similar between the groups (5.1% vs. 5.9% without TIPS, Gray’s test, p = 0.14).
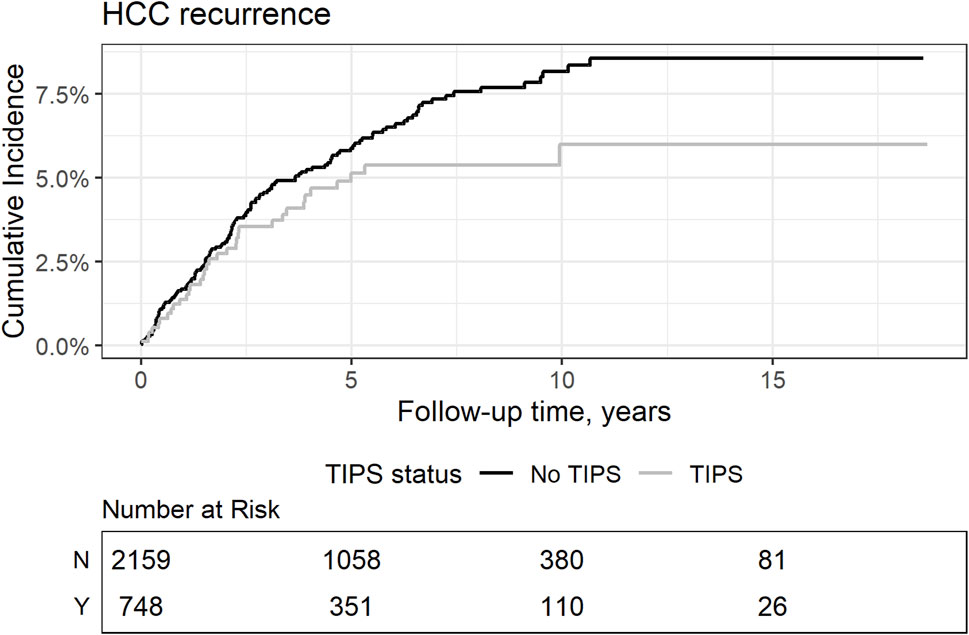
Figure 3. Competed cumulative risk incidence of HCC recurrence comparing patients with and without TIPS. Gray’s test p = 0.14.
Discussion
Our study contributes to the growing body of literature that explores the potential impact of TIPS on HCC. Utilizing a large patient cohort, we present novel insights into the specific advantages conferred by TIPS, especially in the context of tumor burden and survival dynamics among patients awaiting transplantation. A significant finding in our study is that patients with TIPS not only exhibited improved survival while on the waiting list, but also a reduction in the number of HCC nodules. Furthermore, TIPS was not associated with a significant impact on HCC volume or AFP changes.
In line with previous studies [19-24] our findings highlight the benefits of TIPS placement on survival outcomes. This effect may stem from its efficacy in alleviating portal hypertension, enabling concurrent treatment, or reducing bleeding events, potentially serving as a bridge to liver transplantation [22, 25]. Conversely, in cases of advanced HCC, other studies have found that TIPS significantly improved OS by reducing bleeding episodes [26]. However, when assessing TACE efficacy specifically in HCC patients with TIPS, Kuo et al. [10] observed reduced efficacy and shorter overall survival (OS) in the TIPS group. A full understanding of how TIPS influences HCC behavior and treatment response requires further cellular-level investigations that may help establish a conclusive link between TIPS placement and enhanced overall survival.
Prediction models have been developed to examine HCC recurrence after liver transplantation, focusing on factors such as nodule count, size, AFP levels, and vascular invasion, among others [27, 28]. Although the effect of TIPS on posttransplant recurrence has not been extensively explored, our study highlights that TIPS does not affect the risk of HCC recurrence.
Consistent with our results, a meta-analysis of 859 patients by Chen et al. [6] reported that TIPS placement did not increase the risk of HCC development among patients with cirrhosis. This might be due to the reduced proliferative activity of hepatocytes observed after TIPS placement, as reported by Delhaye et al. [29] In contrast, two different studies investigated the impact of TIPS on hepatic blood flow [30, 31] noted increased hepatic blood flow, particularly during the arterial phase of imaging. This observation raises concerns about potential HCC growth subsequent to arterialization of the liver. However, to our knowledge, a direct correlation between TIPS placement and HCC growth has not been established.
The significant difference in OS between the TIPS and non-TIPS groups is noteworthy. This highlights the effectiveness of TIPS as a bridging therapy to enhance life expectancy even in the presence of HCC. The decrease in hemorrhage-related deaths in the TIPS group further supports this notion, indicating the role of this procedure in mitigating the risks associated with portal hypertension.
The precise mechanisms by which TIPS modifies the liver parenchyma and HCC dynamics remain only partially understood. Further histopathological investigations should be performed to understand how TIPS modifies liver vascularization, enabling a more comprehensive treatment strategy for these patients.
Although our study employed propensity score matching, the potential for unmeasured confounders remains a limitation. Moreover, the presence of missing data in our analysis indicates the need for more comprehensive data collection in future studies, including the date of TIPS placement and its correlation with HCC appearance, which could offer insights into the immediate complications of the procedure and potential cancer dissemination in cases of misplacement. Eventually, we acknowledge the heterogenous nature of the SRTR dataset and the potential bias introduced by varying levels of experience and expertise across different centers. Experienced interventional radiology teams could indeed influence the outcomes observed in the TIPS group and future analyses should be include this confounding factor. Future prospective studies are required to validate our findings and to further elucidate the nuanced effects of TIPS on HCC behavior.
In conclusion, our findings support the general beneficial use of TIPS in HCC patients. Although the procedure may stabilize or decrease new tumor formation, it appears that it does not affect HCC growth according to our analyses. Coupled with the observed reduction in hemorrhage-related deaths and improved overall survival, TIPS has emerged as an efficient intervention, particularly for patients awaiting liver transplantation. However, establishing the definitive benefits and risks of TIPS in these patients should be accomplished in future prospective studies.
Data Availability Statement
The data analyzed in this study is subject to the following licenses/restrictions: The data extracted from the SRTR research database is maintained by HHRI solely for the use of the author. The recipient of released data will abide by the terms stated in the Agreement Clauses. Requests to access these datasets should be directed to c29maWEuZWxoYWlqamlAaGN1Z2UuY2g=.
Ethics Statement
The studies involving humans were approved by the Scientific Registry of Transplant Recipients under the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS), through the Chronic Disease Research Group (CDRG) of the Hennepin Healthcare Research Institute (HHRI), with offices at 914 S. 8th Street, Suite S4.100, Minneapolis, Minnesota 55404. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author Contributions
SE led the data collection, analysis, and wrote the manuscript. CT co-developed the study design and contributed to manuscript writing and revisions. SL and BM assisted in data interpretation and provided manuscript feedback. FC and PC reviewed and revised the manuscript, ensuring accuracy and clarity. Each member played a key role in their respective areas, collaboratively advancing the study. All authors contributed to the article and approved the submitted version.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The Swiss National Science Foundation (grant number 182471), the “Fondation Francis and Marie-France Minkoff,” the “Fondation de la Recherche Médicale Carlos et Elsie De Reuter,” the “Fondation Gilles Mentha,” the Swiss Society of Gastroenterology (SGG-SSG), the Swiss Society of Visceral Surgery (SGVC-SSCV), and the Leenaards Foundation (grant number 5489) funded this research.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
AFP: alpha fetoprotein; BMI: body mass index; OS: overall survival; HCC: hepatocellular carcinoma; MELD: Model for End-Stage Liver Disease; SRTR: Scientific Registry of Transplant Recipients; TIPS: transjugular intrahepatic portosystemic shunt; TTV: total tumoral volume.
References
1. García-Pagán, JC, Saffo, S, Mandorfer, M, and Garcia-Tsao, G. Where Does TIPS Fit in the Management of Patients with Cirrhosis? JHEPReport (2020) 2(4):100122. doi:10.1016/j.jhepr.2020.100122
2. Franchis, Rde, Bosch, J, Garcia-Tsao, G, Reiberger, T, Ripoll, C, Abraldes, JG, et al. Baveno VII – Renewing Consensus in portal Hypertension. J Hepatol (2022) 76(4):959–74. doi:10.1016/j.jhep.2021.12.022
3. Thabut, D, and Kudo, M. Treatment of portal Hypertension in Patients with HCC in the Era of Baveno VII. J Hepatol (2023) 78(3):658–62. doi:10.1016/j.jhep.2022.11.019
4. Allaire, M, Rudler, M, and Thabut, D. Portal Hypertension and Hepatocellular Carcinoma: Des Liaisons Dangereuses. Liver Int (2021) 41(8):1734–43. doi:10.1111/liv.14977
5. Hüsing-Kabar, A, Meister, T, Köhler, M, Domschke, W, Kabar, I, Wilms, C, et al. Is De Novo Hepatocellular Carcinoma after Transjugular Intrahepatic Portosystemic Shunt Increased? United Eur Gastroenterol J (2018) 6(3):413–21. doi:10.1177/2050640617732886
6. Chen, B, Pang, L, Chen, HB, Wu, DB, Wang, YH, and Chen, EQ. TIPS Is Not Associated with a Higher Risk of Developing HCC in Cirrhotic Patients: A Systematic Review and Meta-Analysis. J Clin Transl Hepatol (2019) 7(3):232–7. doi:10.14218/JCTH.2019.00007
7. Bañares, R, Núñez, O, Escudero, M, Fernández, C, Vaquero, J, Beceiro, I, et al. Patients with Cirrhosis and Bare-Stent TIPS May Have Increased Risk of Hepatocellular Carcinoma. Hepatology (2005) 41(3):566–71. doi:10.1002/hep.20576
8. Krumeich, LN, Mancinelli, J, Cucchiara, A, Eddinger, K, David Aufhauser, J, Goldberg, DW, et al. Occult Hepatocellular Carcinoma Associated with Transjugular Intrahepatic Portosystemic Shunts in Liver Transplant Recipients. Liver Transplant : official Publ Am Assoc Study Liver Dis Int Liver Transplant Soc (2021) 27(9):1248–61. doi:10.1002/lt.26073
9. Ankoma-Sey, V, Wang, Y, and Dai, Z. Hypoxic Stimulation of Vascular Endothelial Growth Factor Expression in Activated Rat Hepatic Stellate Cells. Hepatology (2000) 31(1):141–8. doi:10.1002/hep.510310122
10. Kuo, YC, Kohi, MP, Naeger, DM, Tong, RT, Kolli, KP, Taylor, AG, et al. Efficacy of TACE in TIPS Patients: Comparison of Treatment Response to Chemoembolization for Hepatocellular Carcinoma in Patients with and without a Transjugular Intrahepatic Portosystemic Shunt. Cardiovasc Intervent Radiol (2013) 36(5):1336–43. doi:10.1007/s00270-013-0698-8
11. R-Project: 2023. The R Project for Statistical Computing. [Accessed 2023 December 18]. Available from: https://www.r-project.org/.
12. Ho, D, Imai, K, King, G, Stuart, E, Whitworth, A, and Greifer, N. MatchIt: Nonparametric Preprocessing for Parametric Causal Inference (2023). Available from: https://cran.r-project.org/web/packages/MatchIt/index.html (Accessed December 18, 2023).
13. Orci, LA, Berney, T, Majno, PE, Lacotte, S, Oldani, G, Morel, P, et al. Donor Characteristics and Risk of Hepatocellular Carcinoma Recurrence after Liver Transplantation. Br J Surg (2015) 102(10):1250–7. doi:10.1002/bjs.9868
14. Samoylova, ML, Dodge, JL, Yao, FY, and Roberts, JP. Time to Transplantation as a Predictor of Hepatocellular Carcinoma Recurrence after Liver Transplantation. Liver Transpl (2014) 20(8):937–44. doi:10.1002/lt.23902
15. Sjoberg, DD, Larmarange, J, Curry, M, Lavery, J, Whiting, K, Zabor, EC, et al. Gtsummary: Presentation-Ready Data Summary and Analytic Result Tables (2023). Available from: https://cran.r-project.org/web/packages/gtsummary/index.html (Accessed December 18, 2023).
16. Kassambara, A, Kosinski, M, Biecek, P, and Fabian, S. Survminer: Drawing Survival Curves Using “Ggplot2” (2021). Available from: https://cran.r-project.org/web/packages/survminer/index.html (Accessed December 18, 2023).
17. Therneau, TM. TL (Original S >R Port and R Maintainer, Elizabeth A, Cynthia C. Survival: Survival Analysis) (2009). Available from: https://cran.r-project.org/web/packages/survival/index.html (Accessed December 18, 2023).
18. Sjoberg, DD, and Fei, T. Tidycmprsk: Competing Risks Estimation (2023). Available from: https://cran.r-project.org/web/packages/tidycmprsk/index.html (Accessed December 18, 2023).
19. Sellers, CM, Nezami, N, Schilsky, ML, and Kim, HS. Transjugular Intrahepatic Portosystemic Shunt as a Bridge to Liver Transplant: Current State and Future Directions. Transplant Rev (2019) 33(2):64–71. doi:10.1016/j.trre.2018.10.004
20. Mumtaz, K, Metwally, S, Modi, RM, Patel, N, Tumin, D, Michaels, AJ, et al. Impact of Transjugular Intrahepatic Porto-Systemic Shunt on post Liver Transplantation Outcomes: Study Based on the United Network for Organ Sharing Database. World J Hepatol (2017) 9(2):99–105. doi:10.4254/wjh.v9.i2.99
21. Laurent, C, Rayar, M, Maulat, C, Muscari, F, Marichez, A, Gregoire, E, et al. Liver Transplantation and Hepatocellular Carcinoma: Is TIPS Deleterious? A Multicentric Retrospective Study of the ARCHET Research Group with Propensity Score Matching. Langenbecks Arch Surg (2023) 408(1):149. doi:10.1007/s00423-023-02875-8
22. Yan, H, Qiu, Z, Xiang, Z, Feng, K, Huang, M, and Gao, F. TIPS Improves Outcomes in Patients with HCC and Symptomatic portal Hypertension: A Multi-Institution Experience. Cancer Imaging (2022) 22(1):13. doi:10.1186/s40644-022-00451-9
23. Norero, B, Bosch, J, Berzigotti, A, and Rodrigues, SG. Transjugular Intrahepatic Portosystemic Shunt in Patients with Hepatocellular Carcinoma: A Systematic Review. United Eur Gastroenterol J (2023) 11:733–44. doi:10.1002/ueg2.12454
24. Luo, SH, Chu, JG, Huang, H, and Yao, KC. Safety and Efficacy of Transjugular Intrahepatic Portosystemic Shunt Combined with Palliative Treatment in Patients with Hepatocellular Carcinoma. World J Clin Cases (2019) 7(13):1599–610. doi:10.12998/wjcc.v7.i13.1599
25. Larrey, E, Cluzel, P, Rudler, M, Goumard, C, Damais-Thabut, D, and Allaire, M. TIPS for Patients with Early HCC: A Bridge to Liver Transplantation. Clin Res Hepatol Gastroenterol (2022) 46(8):101790. doi:10.1016/j.clinre.2021.101790
26. Chen, Y, Ma, X, Zhang, X, Luo, J, An, L, Zhang, Y, et al. Prevention of Variceal Rebleeding in Cirrhotic Patients with Advanced Hepatocellular Carcinoma Receiving Molecularly Targeted Therapy: A Randomized Pilot Study of Transjugular Intrahepatic Portosystemic Shunt versus Endoscopic Plus β-Blocker. Hepatol Int (2022) 16(6):1379–89. doi:10.1007/s12072-022-10388-7
27. Goldaracena, N, Mehta, N, Scalera, I, Sposito, C, Atenafu, EG, Yao, FY, et al. Multicenter Validation of a Score to Predict Prognosis after the Development of HCC Recurrence Following Liver Transplantation. HPB (2019) 21(6):731–8. doi:10.1016/j.hpb.2018.10.005
28. Carr, BI, Guerra, V, Donghia, R, Farinati, F, Giannini, EG, Piscaglia, F, et al. Changes in Hepatocellular Carcinoma Aggressiveness Characteristics with an Increase in Tumor Diameter. Int J Biol Markers (2021) 36(1):54–61. doi:10.1177/1724600821996372
29. Delhaye, M, Louis, H, Degraef, C, Le Moine, O, Devière, J, Gulbis, B, et al. Relationship between Hepatocyte Proliferative Activity and Liver Functional reserve in Human Cirrhosis. Hepatology (1996) 23(5):1003–11. doi:10.1053/jhep.1996.v23.pm0008621125
30. He, J, Li, J, Fang, C, Qiao, Y, and Feng, D. The Relationship and Changes of Liver Blood Supply, Portal Pressure Gradient, and Liver Volume Following TIPS in Cirrhosis. Can J Gastroenterol Hepatol (2022) 2022:7476477. doi:10.1155/2022/7476477
Keywords: liver transplantation, recurrence, survival, progression, hepatocellular carcinoma
Citation: El Hajji S, Lacotte S, Moeckli B, Cauchy F, Compagnon P and Toso C (2024) Transjugular Intrahepatic Portosystemic Shunt Is Associated With Better Waitlist Management of Liver Transplant Candidates With Hepatocellular Carcinoma. Transpl Int 37:12781. doi: 10.3389/ti.2024.12781
Received: 31 January 2024; Accepted: 12 June 2024;
Published: 26 June 2024.
Copyright © 2024 El Hajji, Lacotte, Moeckli, Cauchy, Compagnon and Toso. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sofia El Hajji, c29maWEuZWxoYWpqaUB1bmlnZS5jaA==; Christian Toso, Y2hyaXN0aWFuLnRvc29AaGN1Z2UuY2g=
†ORCID: Beat Moeckli, orcid.org/0000-0002-9020-8416